Atrial Septal Aneurysm-Related Thrombus Causing Ischemic Stroke: A Case Report and Literature Review
by Sabina Scriba1, Caroline Morbach2*, Karl Georg Haeusler3
1Department of Neurology, University Hospital Würzburg, Würzburg, Germany
2Department Clinical Research and Epidemiology, Comprehensive Heart Failure Center and Department of Internal Medicine I, University Hospital Würzburg, Würzburg, Germany
3Department of Neurology, University Hospital Ulm, Ulm, Germany
*Corresponding Author: Caroline Morbach, Department Clinical Research and Epidemiology, Comprehensive Heart Failure Center, Deutsches Zentrum für Herzinsuffizienz Würzburg, Am Schwarzenberg 15, 97078 Würzburg, Germany
Received Date: 11 January 2026
Accepted Date: 15 January 2026
Published Date: 19 January 2026
Citation: Scriba S, Morbach C, Haeusler KG. (2026). Atrial Septal Aneurysm–Related Thrombus Causing Ischemic Stroke: A Case Report and Literature Review. Ann Case Report. 11: 2507. DOI: https://doi.org/10.29011/2574-7754.102507
Abstract
Background: Atrial septal aneurysm (ASA) is associated with recurrent stroke, but the underlying mechanisms are not fully understood. Here, we present a patient with stroke and thrombus formation within an ASA and compare this case to the literature.
Case Presentation: A 61-year-old male presented with acute focal neurological symptoms. Brain imaging revealed an occlusion of the right common carotid artery and multiple bihemispheric lesions. Transesophageal echocardiography (TEE) showed an ASA containing thrombotic material. The patient was treated with full-dose enoxaparin until thrombus resolution, switched to phenprocoumon (target INR 2-3) afterwards, as the ASA could not be treated with an occluding device. Three years after the initial stroke, the patient had not suffered another ischemic event.
Conclusion: Stroke due to an ASA with thrombus formation has rarely been described. This and other cases highlight the importance of cardiac imaging using TEE in cryptogenic stroke. Treatment options include medical therapy, surgery or percutaneous intervention. Decisions should be made on an individual basis as guideline recommendations are lacking.
Keywords: Atrial Septal Aneurysm; ASA; Atrial Thrombus; Ischemic Stroke; Transesophageal Echocardiography; Case Report.
Introduction
Atrial septal aneurysm (ASA) is an abnormality of the atrial septum, usually defined as a saccular deformity protruding at least 10 mm into the left or right atrium [1]. ASA is found in about 2.2% of the general population [2], and the presence of ASA is associated with (recurrent) stroke [3]. Two underlying mechanisms have been reported for ASA-related ischemic stroke: I) the presence of a patent foramen ovale (PFO) promotes the occurrence of paradoxical embolism; II) blood stasis within the aneurysm leading to local thrombus formation and subsequent embolism [4]. However, cases of detected thrombus formation in an ASA in a patient with acute ischemic stroke, as presented here, have rarely been reported [5-7]. Furthermore, we reviewed the existing literature and treatment options.
Case Presentation
A 61-year-old man with a history of hypercholesterinaemia, diabetes mellitus type 2, arterial hypertension and nicotine abuse (approximately 40 pack years) presented with a sudden onset of left-sided hemiparesis to the Department of Neurology, University Hospital Würzburg, Germany. Examination additionally revealed vertical gaze palsy and a multimodal left-sided neglect. Pulse was normofrequent and rhythmic, heart sounds were without murmurs and there were no signs of heart failure. Medication at the time of admission included dapagliflozin, metformin, torasemide and ramipril.
Immediate cranial computed tomography (CT) scan did not show any brain infarction (Figure 1A). CT angiography (CTA) revealed an occlusion of the right common carotid artery (ACC) as well as the proximal right internal carotid artery (ACI) (Figure 1B). Acute stroke treatment included systemic thrombolysis (using 81 mg alteplase) and endovascular treatment with percutaneous transluminal angioplasty and stenting of the right ACC and ACI. The following day, magnetic resonance imaging (MRI) showed an embolic pattern of bihemispheric acute, subacute ischemic lesions and a prior pontine lacunar lesion (Figure 1C-F). The patient was treated with aspirin (100 mg/d) and clopidogrel (75 mg/d) starting 24 hours after thrombolysis.
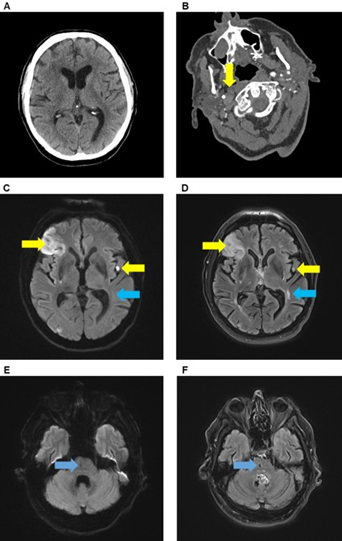
Figure 1: Brain imaging. CT and CT-angiography demonstrating no early signs of ischemic stroke (A) but an occlusion of right common carotid artery (B, yellow arrow) and internal carotid artery. Brain MRI showed multiple new (yellow arrows) and old lesions (blue arrow) in the territory of the left and right medial cerebral artery in DWI (C) and FLAIR sequence (D) as well as a previous lacunar lesion in the right pons (blue arrow) in DWI (E) and FLAIR sequence (F).
No atrial fibrillation (AF) was found within 93 hours of in-hospital monitoring. Transthoracic echocardiography (TTE) revealed a reduced ejection fraction of 25% with global hypokinesia. Transesophageal echocardiography (TEE) showed an ASA bulging into the right atrium (9 x 10 x 9 mm) and containing thrombotic material on the left atrial side (Figure 2). There was no evidence of a PFO with or without Valsalva manoeuvre.
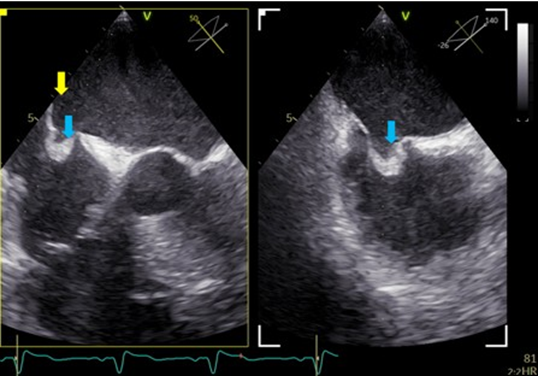
Figure 2: Description of ASA. TOE, mid-oesophageal, 50° and 140°. The two planes show perpendicular views of the ASA. The ASA opens to the left atrium and was filled with thrombus formation (blue arrows) as well as with smoke (yellow arrow). The linked cine loop shows the same views in the moment when rightheart contrast agent was administered. There was no contrast agent detectable in the left atrium, thus excluding an interatrial shunt.
Immediately after TEE, enoxaparin (0.7 mg twice daily) was given subcutaneously for 4 weeks in addition to aspirin after interdisciplinary discussion, while clopidogrel was stopped to reduce the overall bleeding risk. After rehabilitation and 4 weeks after stroke onset, no thrombotic material was visible during a control TEE. However, after thrombus resolution the ASA was revealed to cover the whole interatrial septum (Figure 3). We discussed the implantation of an atrial occluder device but concluded that it would not sufficiently cover the large ASA and, subsequently, might even increase the risk of re-thrombus formation. Thus, anticoagulation was switched to phenprocoumon (with a target-INR of 2-3) acetylsalicylic acid was discontinued. During follow-up visits up to 36 months after the index stroke, the patient did not report any signs of recurrent stroke.
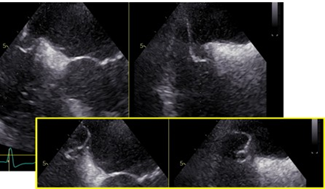
Figure 3: Resolution of thrombus. TOE, mid-oesophageal, 35° and 125°. The two planes show perpendicular views of the ASA. There is no thrombus left. With changing pressure in both atria, the interatrial septum floats into the left atrium, revealing the ASA covering the whole septum (yellow box).
Discussion
A review of existing literature identified three other cases of a thrombus in ASA [5-7], and one case of a thrombus in an atrioventricular septal aneurysm [8] as likely causes of acute ischemic stroke. The characteristics of the aforementioned case reports are summarised in (Table 1). Other reports of thrombus formation in ASA exist [1], however without describing the clinical relevance, consecutive embolic events or treatment of ASA.
|
Chammas et al. 1995 [5] |
Lin et al. 1995 [8] |
Salazar et al. 2003 [6] |
Miyazaki et al. 2005 [7] |
Present case |
|
|
Sex |
Female |
Female |
Female |
Male |
Male |
|
Age at event |
72 years |
19 years |
14 years |
89 years |
61 years |
|
Cardiovascular risk factors |
Hypercholesterinaemia |
None |
None |
Atrial fibrillation |
Arterial hypertension, diabetes mellitus type 2, hypercholesterinaemia, nicotine abuse |
|
Stroke symptoms |
Left-sided hemiparesis, apraxia, aphasia, dementia |
Left-sided hemiparesis |
Visual loss of the left eye |
Left-sided hemiparesis |
Left-sided hemiparesis |
|
Brain imaging |
CT, MRI |
CT, MRI |
Modality not reported |
CT, MRI angiography |
CT, CT angiography, MRI |
|
Infarct localisation |
Multiple bihemispheric lesions |
Single lesion of right basal ganglia |
Cilioretinal artery |
Middle cerebral artery |
Multiple bihemispheric lesions |
|
Acute stroke Treatment |
None |
None |
Anticoagulant therapy (not specified) |
None |
Systemic thrombolysis using alteplase, endovascular treatment |
|
Cardiac imaging |
TTE, TEE |
TTE, TEE |
TTE, TEE |
TTE, TEE |
TTE, TEE |
|
ASA (diameter 15 mm) containing thrombotic mass (5x13 mm) |
Atrioventricular septum aneurysm with intraaneurysmatic mass |
ASA (diameter 10 mm) containing thrombotic mass |
ASA and a floating thrombotic mass in the left atrium |
ASA (9x10x9 mm) containing thrombotic material |
|
|
PFO |
No |
No |
Yes |
Yes |
No |
|
Treatment |
None |
Surgical resection of aneurysm and thrombus |
Surgical resection of aneurysm and thrombus |
None |
None |
|
Antiplatelets/ Anticoagulation |
Intravenous Heparin (duration not specified) |
None |
Oral anticoagulation for 6 months (dose not specified) |
Warfarin for 4 weeks (dose not specified) |
Full-dose heparin and |
|
Subsequent ASS 300 mg daily |
phenprocoumon (target INR 2-3, lifelong) |
||||
|
Outcome |
Follow-up 8 months: No evidence of thrombus in TEE, no further events |
Hemiparesis was mostly resolved at hospital discharge, no follow up reported |
Follow-up 24 months: No further events |
Follow-up 4 weeks: No evidence of thrombus in TEE, no further events |
Follow-up 4 weeks: Resolution of thrombus in TEE, follow-up 36 months: no further events |
|
Abbrevations: ASA - atrial septal aneurysm; MRI - magnetic resonance imaging; PFO - patent foramen ovale; TEE - transesophageal echocardiography; TTE - transthoracic echocardiography. |
|||||
Table 1: Case reports of stroke related to a thrombus within an atrial aneurysm [5-8].
The prevalence of ASA within the general population is about 2.2%, whereas prevalence in patients with ischemic stroke has been reported to be 8% in retrospective single-centre studies [2, 4]. Within this stroke population, the occurrence of ASA-related thrombi appears to be rare, with a reported prevalence of 1% in a prospective multi-centre study [1]. ASA is more common in patients under 55 years with embolic stroke of undetermined source (ESUS), while atrial thrombus is more frequent in older individuals [9]. Atrial aneurysms appear to be either congenital or may form due to pressure differences between the left and right atrium [4]. The cohort of patients with thrombus in atrial aneurysms ranges from teenagers to elderly patients [5-8].
ASA is often linked with other atrial defects, such as PFO [2, 3]. Both PFO and ASA correlate with stroke risk and the combination of both further increases the risk of stroke [10]. Notably, ASA is a stronger predictor of recurrent stroke than PFO size [3]. Patients with ASA >10 mm in diameter have an 8-fold higher risk of stroke than those with a smaller ASA according to a retrospective singlecentre study [10]. ASA may act as an arrhythmogenic focus, as several observational studies have shown an increased prevalence of atrial tachyarrhythmia in patients with ASA [4]. While our patient had neither other septal abnormalities nor AF, two of the three other patients reported in Table 1 were diagnosed with PFO and AF was reported in one case [6, 7].
Previous studies highlight the higher sensitivity of TEE for detection of ASA compared to TTE [11], with TTE missing ASA in 47% of cases in one study [1]. TEE appears to be more reliable than cardiac computed tomography in detecting ASA, while cardiac computed tomography detects atrial thrombi more efficiently [11]. However, TEE is currently not recommended for diagnostic workup in all stroke patients as there is a weak correlation between cardiac abnormalities and stroke [9]. Notably, the European Association of Cardiovascular Imaging recommends the use of contrast-enhanced TTE to rule out atrial septal abnormalities in patients with stroke and refers to TEE in the case of suspicious findings [11]. The European Society of Cardiology has proposed assessing thromboembolic risk of ASA and PFO in combination with the history of venous thromboembolism, age of the patient and the risk of paradoxical embolism (RoPE) score [12].
Currently, there are no evidence-based guidelines on the therapeutic management of ASA-related thrombus. Treatment may include antiplatelet therapy, anticoagulation, surgical closure or percutaneous intervention [4]. Notably, residual cardiac thrombus is linked to poor clinical outcomes in patients with ischemic stroke [13]. In case of left atrial thrombi, anticoagulation using vitamin K antagonists or direct oral anticoagulants (DOACs) should be considered on an individual basis [14], and heparin may be an option [4]. A recent meta-analysis of 6 studies with a total of 353 patients concluded that DOACs were more effective than warfarin in dissolving left atrial appendage thrombi in AF patients with fewer bleeding events occurring [15]. It remains unclear whether these results can be transferred to ASA-related thrombi. Under anticoagulation, TEE follow-ups until thrombus resolution are recommended [14]. Other literature reviews on ASA suggest considering occlusion after thrombus resolution, especially when ASA and PFO coexist [3] and recommending constant anticoagulation to reduce risk of subsequent thromboembolic events, when occlusion is not possible [4]. In two of the case reports, surgery was performed to retrieve the thrombus and treat the aneurysm. In both cases patients were young, and surgery was seen as a valuable alternative to long-term anticoagulation [6, 8].
So far, there are no randomised studies comparing surgery as an alternative to catheter-based occlusion of ASA.
Our reported case of stroke due to thrombus formation in ASA highlights the importance of cardiac imaging using TEE in otherwise cryptogenic stroke. There are no general treatment recommendations or guidelines on ASA-related thrombus formation in acute stroke patients. Therefore, treatment should be individualised after interdisciplinary discussion and carefully discussed with the patient.
Learning points
- Atrial septal aneurysm as an abnormality of the atrial septum can in rare instances contain thrombotic material and lead to recurrent ischemic strokes.
- Atrial septal aneurysms are best diagnosed through transesophageal echocardiography, which also facilitates the assessment of their contents.
- Treatment of thrombotic material in atrial septal aneurysms should involve an interdisciplinary team and options discussed on an individual basis.
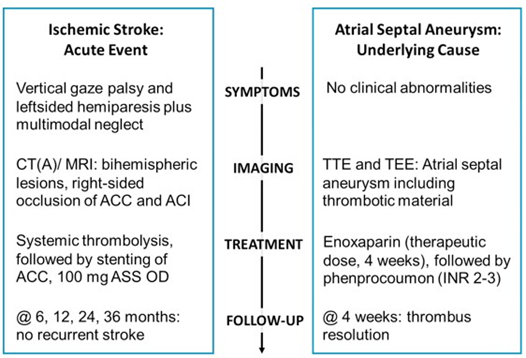
Summary figure
Statement of consent: Informed written consent was obtained from the patient for the submission and publication of this case report in accordance with COPE guidelines.
Data availability: The data underlying this article will be shared on reasonable request to the corresponding author.
Author contributions: KGH and CM were involved in the treatment of the patient. SS drafted the manuscript, figure 1 and table 1. CM was responsible for drafting figure 2 and 3. Both KGH and CM reviewed the work. All the authors have given final approval of the version to be published.
Funding: None declared.
Conflict of Interest: None declared.
Acknowledgements: None declared.
References
- Mügge A, Daniel WG, Angermann C, Spes C, Khandheria BK, et al. (1995) Atrial septal aneurysm in adult patients: A multicenter study using transthoracic and transesophageal echocardiography. Circulation. 91: 2785-2792.
- Agmon Y, Khandheria BK, Meissner I, Gentile F, Whisnant JP, et al. (1999) Frequency of atrial septal aneurysms in patients with cerebral ischemic events. Circulation. 99: 1942-1944.
- Mas JL, Saver JL, Kasner SE, Nelson J, Carroll JD, et al. (2022) Association of atrial septal aneurysm and shunt size with stroke recurrence and benefit from patent foramen ovale closure. JAMA Neurology. 79: 1175-1179.
- Shah D M. (2012) A look at atrial septal aneurysm. Journal of Cardiovascular Medicine. 10: 1-6.
- Chammas E, Trinca M, Goullard L, Leys D, Houdas Y. (1995) Multiple cerebral infarcts associated with an atrial septal aneurysm: Superimposed thrombus detected by transesophageal echocardiography. Angiology. 46: 327-331.
- Salazar J, Gutierrez A, Cay E, Ballester C, Salazar JJ, et al. (2003) Cerebral embolism and thrombus in a membranous interventricular septal aneurysm. Annals of Thoracic Surgery. 76: 286-287.
- Miyazaki S, Hirai T, Hosokawa N, Hattori E, Komura M, et al. (2005) Impending paradoxical cerebral embolism in a patient with atrial septal aneurysm. Circulation Journal. 69: 246-248.
- Lin JM, Hwang JJ, Chiu IS. (1995) Cerebral embolism from the thrombus in the atrioventricular septal aneurysm. Cardiology. 86: 441443.
- McGrath ER, Paikin JS, Motlagh B, Salehian O, Kapral MK, et al. (2014) Transesophageal echocardiography in patients with cryptogenic ischemic stroke: A systematic review. American Heart Journal. 168: 706-712.
- Cabanes L, Mas JL, Cohen A, Amarenco P, Cabanes PA, et al. (1993) Atrial septal aneurysm and patent foramen ovale as risk factors for cryptogenic stroke in patients less than 55 years of age: A study using transesophageal echocardiography. Stroke. 24: 1865-1873.
- Cohen A, Donal E, Delgado V, Pepi M, Tsang T, et al. (2021) EACVI recommendations on cardiovascular imaging for the detection of embolic sources: Endorsed by the Canadian Society of Echocardiography. European Heart Journal Cardiovascular Imaging. 22: e24-e57.
- Ntaios G, Baumgartner H, Doehner W, Donal E, Edvardsen T, et al. (2024) Embolic strokes of undetermined source: A clinical consensus statement of the ESC Council on Stroke. European Heart Journal. 45: 1701-1715.
- Zhang T, Zhou H, Yang J, Zhou Y, Chen Y, et al. (2024) Presence of residual cardiac thrombus predicts poor outcome in cardioembolic stroke after reperfusion therapy. Journal of the American Heart Association. 13: e032200.
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, et al. (2021) 2020 15. ESC guidelines for the diagnosis and management of atrial fibrillation. and safety profile of novel oral anticoagulants in the treatment of left European Heart Journal. 42: 373-498.
- Dong SJ, Luo CY, Xiao CL, Zhang FZ, Li L, et al. (2022) Efficacy atrial thrombosis: A systematic review and meta-analysis. Current Therapeutic Research Clinical and Experimental. 96: 100670.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.