APR is the Preferred Option for the Ultra low Anterior Resection, 5 cm and Below
Haitham Akram Saimeh*
*Corresponding Author: Haitham Akram Saimeh, King Faisal Speciality Hospital and Research Centre, Saudi Arabia.
Received Date: 05 October 2021
Accepted Date: 08 October, 2021
Published Date: 14 October 2021
Citation: Saimeh HA. (2021) APR is the Preferred Option for the Ultra ow Anterior Resection, 5 cm and Below. Ann Case Report 6: 705. DOI: 10.29011/2574-7754.100705
Introduction
Colorectal cancer is known to be a lethal diseases which is influenced by both environmental as well as genetic factors. According to the world health organization, colorectal cancer is the third most commonly diagnosed cancer in males and the second in females [1]. There are geographical differences and this is attributed to differences in in dietary and environmental exposures as well as low socioeconomic status which contributes to lower rates of screening .
Case Presentation
A 65 year old male patient with previous history of controlled hypertension, was admitted under neurology care after experiencing a history of right sided weakness and an episode of fall. During screening, abdominal CT scan showed colon mass with suspicious features, of an irregular mass infiltrating the wall of the lower rectum few centimeters from the anal verge, distended and constipated proximal large bowel loops, however the patient only complained of chronic constipation, no any other symptoms. After a colonoscopy and biopsy were done, findings showed that there is an adenocarcinoma which is moderately differentiated. Brain mass biopsy revealed that there is a metastatic adenocarcinoma, which is consistent with colon primary (Figure 1).
On physical examination, abdomen was soft, lax and lower left quadrant mass, digital rectal examination couldn’t be done because it’s painful. By these findings the patient was diagnosed as a colon cancer patient and management plan was set based on the findings. Below is a brain CT, demonstrating brain tumor (Figure 2).
Discussion
There are several colorectal cancer presentations , including suspicious symptoms or some patients maybe asymptomatic which are discovered incidentally by routine screening and there are other unusual presentations including fever of unknown origin , or discovered by incidental metastasis .Colorectal cancer diagnosis is made by both histological together with colonoscopic findings as well as laboratory tests as tumor markers including serum levels of CEA have a great value in the prognosis and follow up of patients diagnosed with colorectal cancer [2]. Clinical staging is important in the clinical evaluation , this is done via physical examination together with CT of the abdomen , chest and pelvis. In the late course of the disease, brain metastasis will develop late, prognosis in such cases is considered poor, however with the new systemic therapies, early detection and treatment of brain metastases may end up in improving the outcome. Brain metastasis in colorectal cancer in quiet rare compared to manifestations from other tumors as malignant melanoma, lung and breast cancers. Brain metastases usually results from hematogenous spread through the Baston vertebral venous plexus [3]. Treatment modalities for brain metastases from colorectal cancer doesn’t differ from primary brain lesions , best survival improvement was seen in patients who have conducted full surgical resection followed by whole – brain radiation.
Conclusion
Survival of patients with brain metastases is dismal, at a reported median of less than 3 months , but since brain metastases is considered to be rare therefore routine brain screening is not considered cost effective in improving the patients overall survival rate . For better long-term survival, early diagnosis followed by aggressive treatment set by a multi -disciplinary team is the gold standard choice.
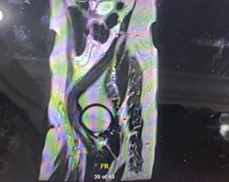

Figure 1: Abdominal CT scan showed colon mass with suspicious features.
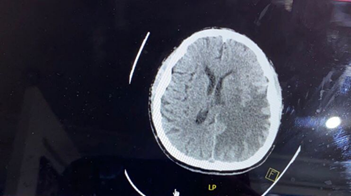
Figure 2: Brain CT, demonstrating brain tumor.
References
- Rawla P, Sunkara T, Barsouk A. (2019) Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol. 14: 89-103.
- Damiens K, Ayoub JP, Lemieux B, Aubin F, Saliba W, et al. (2012) Clinical features and course of brain metastases in colorectal cancer: an experience from a single institution. Curr Oncol. 19: 254-258.
- Mongan JP, Fadul CE, Cole BF, Zaki BI, Suriawinata AA, et al. (2009) Brain metastases from colorectal cancer: risk factors, incidence, and the possible role of chemokines. Clin Colorectal Cancer. 8: 100-105.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.