An Innovation for Prevention and Treatment of Gastroesophageal Reflux Disease, Akram’s Dietary Regime-Mini Review
by Muhammad A Randhawa1*, Sadia A Khan2, Tayyab S Akhter3, Muhammad Umar4
1Department of Pharmacology, Rawalpindi Medical University, Rawalpindi, Pakistan
2Department of Family Medicine, Rawalpindi Medical University, Rawalpindi, Pakistan 3Department of Gastroenterology, Rawalpindi Medical University, Rawalpindi, Pakistan
4Department of Medicine, Rawalpindi Medical University, Rawalpindi, Pakistan
*Corresponding author: Muhammad A Randhawa, Department of Pharmacology, Rawalpindi Medical University, Rawalpindi, Pakistan
Received Date: 20 December, 2024
Accepted Date: 30 December, 2024
Published Date: 07 January, 2025
Citation: Randhawa MA, Khan SA, Akhter TS, Umar M (2025) An Innovation for Prevention and Treatment of Gastroesophageal Reflux Disease, Akram’s Dietary Regime-Mini Review. J Family Med Prim Care Open Acc 9: 271. https://doi.org/10.29011/2688-7460.100271
Abstract
Introduction: Gastro-Oesophageal Reflux Disease (GERD) is becoming a problem for medical profession. Proton Pump Inhibitors are prescribed as first line therapy, but their prolonged use, mostly needed, causes achlorhydria leading to infections and anaemia, etc. Irregular dietary habit is reported to have strongest association with prevalence of GERD. Because a meal when stomach already contains food causes more release of acidic juice and dilates upper stomach, which trigger reflux. It is suggested that a suitable interval between meals, i.e., two meals a day, morning and evening, with only liquids in between (Akram’s life-style) would prevent and treat GERD. Methods: In present work few studies pertaining to practice of Akram’s life-style have been summarized. Initially, a cases report (n=4) and a pilot study (n=20) linked to practice of proposed dietary regime for 2 weeks. Then a single case study, with severe GERD, who continued suggested dietary regime for 7 years. Finally, a clinical study (n=60) conducted at Gastroenterology Unit of a teaching hospital and efficacy of suggested regime evaluated against GERD symptoms after 2 weeks. Results: All patients of initial cases report and 75% of pilot study were relieved of GERD symptoms in 2 weeks. One patient who continued our dietary regime for long time, mostly remained symptom free. Endoscopy done after 7 years showed competent lower oesophagus, no inflammation and Barrett. Lastly, clinical study demonstrated marked improvement (P=0.000) in GERD symptoms when evaluated after two weeks of adaptation of our dietary regime, without medication. Conclusions: Regular practice of Akram’s life-style, two meals a day with only fluids in between, prevents episodes of gastric acid reflux due to irregular feasts and is proposed as a useful alternate for prevention and treatment of GERD.
Keywords: Gastroesophageal reflux disease; Akram’s lifestyle; Two meals daily; Only fluids in between; Remedy for GERD
Introduction
GERD is becoming a challenge for medical profession because its prevalence is increasing, requires long-term risky drug-therapy and/or surgical interventions and the recurrence rate is high with any mode of treatment. Worldwide prevalence of GERD was found to be 13.98%, varying from 4.16% in China to 22.4% in Turkey [1]. In South Punjab, Pakistan, a study reported prevalence rate of 26.6% [2]. A Japanese study reported that irregular dietary habits had the strongest association with GERD, and Proton Pump Inhibitors (PPIs) in usual doses could not control the disease [3]. Because a meal on top of the meal causes more release of acidic gastric juice and dilates upper stomach, which generate Transient Lower Oesophageal Sphincter Relaxations (TLESRs) and trigger reflux [4]. Repeated acid refluxes damage lower oesophagus, which becomes inflamed and ulcerated; causing heart burn, sore throat, dysphagia, metaplasia, hyperplasia and cancer [5].
PPIs are considered safe and given as first-line drugs for management of GERD. But their prolonged use, which is mostly required, causes severe achlorhydria leading to serious infections such as diarrhoea, pneumonia and candidemia. Their long-term use also causes deficiency of Vitamin B12 and minerals (such as iron, calcium and magnesium), linked to anaemia, osteoporosis, spontaneous fractures and cardiac arrhythmia. Moreover, the recurrence rate is high after they are discontinued [6]. In a clinical study conducted on more than 2600 patients who had primary laparoscopic anti-reflux surgery for GERD, the recurrence rate was reported to be 17.7%; and they were treated with long-term PPIs or H-2 receptor antagonists (83.6%), whereas16.4% underwent secondary anti-reflux surgery [7]. A systemic review of 81 studies, 4584 reoperations in 4509 patients, reports that frequent reflux and dysphagia were the most prevalent indications for surgical reintervention, intraoperative complications occurred in 21.4% and postoperative complications in 15.6% with an overall mortality rate of 0.9% [8].
Considering the pathophysiology of GERD and its strong association with irregular diet, a new life-style change, “Akram’s life-style”, two moderate regular meals a day, morning and evening, with only liquids (Water, fruit juice, tea, coffee and milk, etc.) during the intervening period whenever patient feels hungry or thirsty, has been suggested as an alternate remedy for the management of GERD.
Methods
The present mini-review is a summary of some studies relevant to practice of Akram’s life-style for treatment of GERD. Firstly, a cases report (n=4) to demonstrate benefits of the practice of our suggested dietary regimen for 2-3 weeks [9]. Secondly, a pilot study conducted on endoscopically diagnosed GERD patients (n=20), who practiced our dietary schedule for two weeks [10]. Thirdly, report of a patient shown to have inflammation, erosions, Schatzki‘s ring and small Barrett at gastroesophageal junction on endoscopy, continued our dietary regimen for long time and endoscopy done after 7 years to see the prognosis [11]. Finally, a clinical study (n=60) conducted at Gastroenterology Unit of Rawalpindi Medical University (RMU), to evaluate the effect of Akram’s life-style on typical GERD symptoms, using questionnaire with Yes/No response and VAS [12].
Results
Results of studies included in present work are summarized in Table 1. In initial cases report (n=4), all patients were relieved of GERD symptoms in 2-3 weeks. In pilot study on 20 patients, 15 (75%) were free of GERD symptoms and 2 (10%) showed partial improvement, without medication in 2 weeks (Table 2). One patient, endoscopically depicted to have inflammation, erosions and small Barrett at gastroesophageal junction, continued our dietary regimen for long time and remained symptom free. Occasional heart burn due to breach in dietary protocol was relieved with antacids for 2-3 days. Endoscopy done after 7 years showed competent lower oesophagus, no inflammation, Schatzki‘s ring, or Barrett (Figures 1 and 2). Lastly, the clinical study (n=60) demonstrated marked improvement in GERD symptoms (P=0.000) when evaluated after two weeks of Akram’s life-style adaptation (Tables 3 and 4, showing the results of Yes/No response and VAS, respectively).
|
S. No. |
Study |
Outcome |
|
1 |
Initial cases report (n=4) |
All four patients of GERD were relieved of reflux symptoms within 2-3 weeks without medication. |
|
2 |
Pilot study (n=20) |
Recovery rate in GERD symptoms (Los Angles grade a, b & c) after 2 weeks was 75%, while 10% showed partial benefit. |
|
3 |
Long term practice of Akram’s lifestyle (n=1) |
One patient, who had erosions and Barrett in lower esophagus continued our dietary regimen for long time and remained symptom free. Endoscopy done after 7 years showed competent lower esophagus, no inflammation or Barrett. |
|
4 |
Clinical study (n=60) |
Demonstrated marked improvement in GERD symptoms (P=0.000) when evaluated after two weeks of Akram’s life-style adaptation. |
Table 1: Studies relevant to practice of Akram’s Life-style for treatment of GERD.
|
LA grade |
Overall response |
||||
|
a |
10 |
50% |
Improved |
15 |
75% |
|
b |
6 |
30% |
Partial improvement |
2 |
10% |
|
c |
4 |
20% |
No Improvement |
3 |
15% |
Table 2: Summary of the results of 20 cases of GERD (Pilot study) who took the suggested meal regime, showing frequency of LA grades and overall response rate.
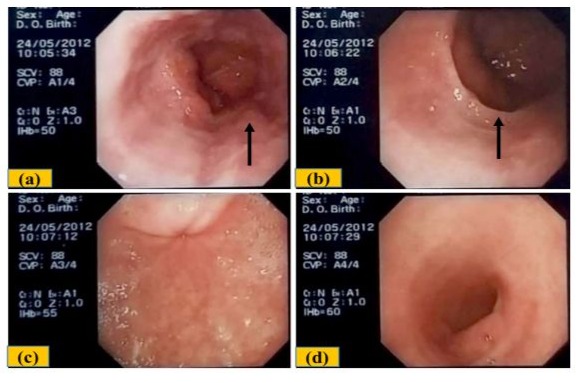
Figure 1. (a) Inflammation and erosions at gastroesophageal junction and a small Barrett’s (Arrow). (b) Incomplete Schatzki’s ring (Arrow). (c) Moderate diffuse erythema with mild erosions in the antrum. (d) Pylorus and initial part of duodenum appear normal.
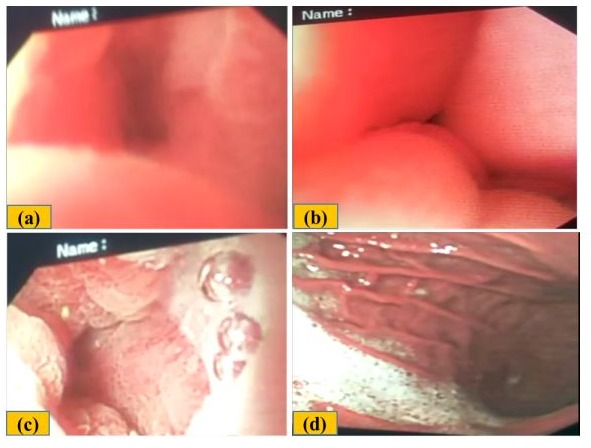
Figure 2: (a & b) Normal gastroesophageal junction, no erosions, Barrett, or Schatzki’s ring (c) Erosions in antrum, possibly age related (d) Normal pylorus.
|
Gastrointestinal Symptoms |
Before Intervention Y/N [n=60], Y% |
After Intervention !Y/N [n=45], Y% |
Improvement (Reduction) and (% reduction) in Y |
|
Heart burn |
56/4, (93.3%) |
13/32, (28.8%) |
64.5 (69.1%) |
|
Reflux |
52/8, (86.6%) |
6/39, (15.4%) |
71.2 (82.2%) |
|
Nausea |
47/13, (78.3%) |
5/40, (11.1%) |
67.2 (85.8%) |
|
Vomiting |
24/36, (40%) |
4/41, (8.8%) |
31.2 (72%) |
|
Dysphagia |
35/25, (58%) |
3/42, (6.6%) |
51.4 (88.6%) |
Table 3. Yes/No [Y/N] response to gastrointestinal symptoms, before and after intervention. Improvement was estimated from % reduction in Y response, demonstrating marked reduction (69.1 to 88.6 %) in Y-response.
|
Symptoms |
VAS score before (Mean ± SD) |
VAS score after (Mean ± SD) |
P value |
|
Heart burn |
7.75 ± 1.91 |
0.83 ± 1.43 |
0.000 |
|
Reflux |
5.77 ± 3.09 |
0.64 ± 1.55 |
0.000 |
|
Nausea |
5.28 ± 3.37 |
0.13 ± 0.45 |
0.000 |
|
Vomiting |
2.38 ± 3.38 |
0.04 ± 0.20 |
0.000 |
|
Dyspepsia |
3.13 ± 3.31 |
0.09 ± 0.35 |
0.000 |
Table 4. Cumulative VAS of various gastrointestinal symptoms of GERD, before and after intervention (n=60 and 45, respectively), showing highly significant reduction in severity of GERD symptoms (P=0.000).
Discussion
Irregular dietary habits are reported to have the strongest association with GERD [3]. Because intake of meal when stomach already has food causes another surge in gastric acid secretion and distention of the upper stomach, which trigger generation of Transient Lower Oesophageal Sphincter Relaxations (TLESRs). TLESRs are important cause of gastric acid reflux. Moreover, meal during fasting phase prevents development of migrating myoelectric complexes (MMC) in distal stomach which also travel to intestines. MMCs develop during fasting, clear stomach of debris and propel food onwards (Figure 3). Poverty of MMCs delays gastric emptying and favours reflux [13].
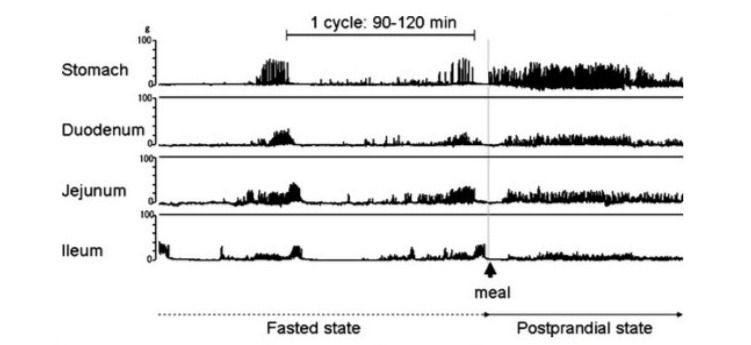
Figure 3: During fasting, cyclic contractions & relaxations at regular intervals (MMCs), propel food onwards. In post-prandial state; irregular tonic contractions, prevent propulsion of food [13].
Akram’s life-style for prevention and treatment of GERD involves two meals a day with only liquids in between. Sufficient interval between two meals avoids triggering of TLESRs, an important cause of reflux, and allows stomach and upper intestines to empty, favouring onward flow of food, minimizing chances of reflux. Liquids allowed between two meals, leave the stomach fast and are least likely to induce reflux. Moreover, enough fasting period between meals favours development of Migrating Myoelectric Complexes (MMC) in distal stomach, which propel food onwards, avoid delay in gastric emptying and prevent reflux.
Why two meals a day? Emptying time of stomach is 4 to 5 hours and that of upper intestines is also about 4 to 5 hours [14]. Therefore, suitable interval between 2 meals is around 8-10 hours, i.e., morning and evening. Intake of food when stomach and upper intestines are empty is least likely to induce reflux (Figure 4a).
Why only liquids during interval? Liquid meal leaves stomach fast, transit half-time is 10 to 30 min. While solids diet is slow to leave, transit half-time is 2 to 3 hours. Liquid meal is unlikely to delay gastric emptying and trigger reflux (Figure 4b) [15].
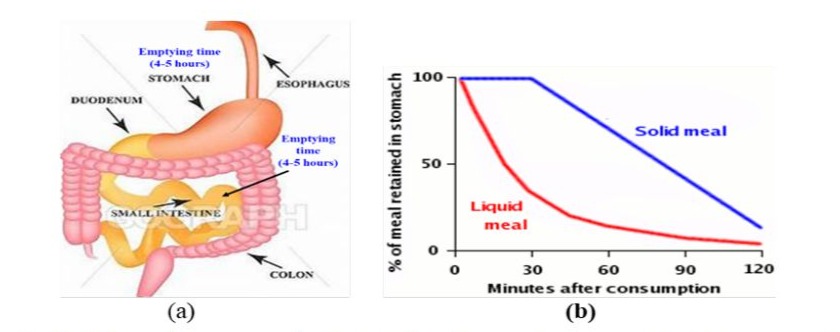
Figure 4: (a) Suitable interval between two meals is about 8-10 hours, when stomach and upper part of intestines are empty [14]. (b) Liquid meal is fast to leave stomach and solid food takes longer [15].
Regular moderate two meals a day work like drugs for GERD. Avoiding meal at top of meal prevents hyperacidity (Like PPIs or other anti-secretory drugs). Sufficient fasting interval favours development of MMCs, which propel food onwards, avoid delay in gastric emptying (like Prokinetic drugs).
Akram’s lifestyle is very cost effective in the management of GERD. Avoids the use of medications. Billions of dollars are being spent worldwide on the purchase of PPIs and other drugs for the treatment of GERD. Two moderate meals a day would also reduce the daily expenses on food. Saving of even one dollar a day per person would mount to conservation of millions of dollars in the annual expenses on food.
Historical
Suggestion to take regular meal and avoidance of intake of meal when stomach is full of food is linked to the advice of Luqman the Wise (Allah be pleased from him), 1100 BC, to his son, mentioned in reference to the explanation of a versus of the Holy Quran: Luqman (Allah be pleased from him) said to his son, ‘Oh my son, do not eat anything after you have taken to your satisfaction. If you leave it for a dog is better than you eat it’ [16].
In the Noble Quran it is narrated that in the hereafter, the people of paradise will be served two meals a day, morning and evening: “They shall not hear therein (in Paradise) any ‘Laghw’ (dirty, false, evil, vain talk), but only ‘Salam’ (salutations of peace). And they will have their sustenance (food) morning and evening” [17].
Conclusions
Prevalence of GERD is increasing due to changes in dietary habits, Drugs used for GERD are becoming ineffective and their longterm use results into serious complications. Akram’s life-style,
i.e., two meals a day with only fluids in between, controls acid refluxes by reducing development of TLESR’s and acid surges and by favouring occurrence of MMCs. Hopefully, it would serve as a useful alternate to risky drug treatment. Further studies with larger sample are suggested for the confirmation of the results of present work.
References
- Nirwan JS, Hasan SS, Babar ZU, Conway BR, Ghori MU (2020) Global Prevalence and Risk Factors of Gastro-oesophageal Reflux Disease (GORD): Systematic Review with Meta-analysis. Sci Rep 10: 5814.
- Rasool MF, Sarwar R, Arshad MS, Imran I, Saeed H, et al. (2021) Assessing Frequency & Risk Factors Associated with Gastroesophageal Reflux Disease (GERD) in Southern Punjab, Pakistan. Risk Manag Health Policy 14: 4619-4625.
- Yamamichi N, Mochizuki S, Asada-Hirayama I, Mikami-Matsuda R, Shimamoto T, et al. (2012) Lifestyle factors affecting gastroesophageal reflux disease symptoms: a cross-sectional study of healthy 19864 adults using FSSG scores. BMC Med 10: 45.
- Han SH, Hong SJ (2012) Transient lower esophageal sphincter relaxation and the related esophageal motor activities. Korean J Gastroenterol 59: 205-210.
- Azer SA, Hashmi MF, Reddivari AKR (2024) Gastroesophageal Reflux Disease (GERD) [Updated 2024 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
- Koyyada A (2021) Long-term use of proton pump inhibitors as a risk factor for various adverse manifestations. Therapie 76: 13-21.
- Maret-Ouda J, Wahlin K, El-Serag HB, Lagergren J (2017) Association Between Laparoscopic Antireflux Surgery and Recurrence of Gastroesophageal Reflux. JAMA 318: 939-946.
- Furnée EJ, Draaisma WA, Broeders IA, Gooszen HG (2009) Surgical reintervention after failed antireflux surgery: a systematic review of the literature. J Gastrointest Surg 13: 1539-1549.
- Randhawa MA, Yar T, Gillessen A (2013) An effective and physiological lifestyle change for management of gastroesophageal reflux diseasecases report. J Ayub Med Coll Abbottabad 25: 206-207.
- Randhawa MA, Mahfouz SA, Selim NA, Yar T, Gillessen A (2015) An old dietary regimen as a new lifestyle change for Gastroesophageal reflux disease: A pilot study. Pak J Pharm Sci 28: 1583-1586.
- Randhawa MA, Khan SA, Naseer A, Baqai MT (2024) NonPharmacological approach for management of gastroesophageal reflux disease. Pak J Med Sci 40: 549-551.
- Khan SA, Randhawa MA, Baqai MT (2024) Benefits of long-term practice of a new life-style change for management of GERD- a case report. Presented as poster in BPS-2022, 13-15 September, Liverpool, UK.
- Khan SA, Khan J, Randhawa MA (2023) Clinical study for the evaluation of a new life-style, Akram’s Life-style, for management of GERD). Presented in 19th World Congress of Basic & Clinical Pharmacology (IUPHAR), Glasgow, UK, 2-7 July 2023 as a poster (No.827).
- Deloose E, Janssen P, Depoortere I, Tack J (2012) The migrating motor complex: control mechanisms & role in health & disease. Nat Rev Gastroenterol Hepatol 9: 271-285.
- Degen LP, Phillip SF (1996) Variability of gastrointestinal transit in healthy women and men. Gut 39: 299-305.
- Camilleri M, Malagelada JR, Brown ML, Becker G, Zinsmeister AR (1985) Relation between antral motility and gastric emptying of solids and liquids in humans. Am J Physiol 249: G580-G585.
- Al-Qortoby AAM (2006) Verse 31, Chapter 7 (Al-Ahraf). In Al-Jamih Al-Ahkam Al-Qoran, Vol 9. Al Resalah Publishers, Beirut, Lebanon. Pp: 196-202.
- Al-Hilali MT, Khan M 1404 (H) [1983 (G)], Verse 62, Chapter 19 (Maryam). In Translation of the meanings of The Noble Qur‘an in the English language. King Fahd Complex for the Printing of the Holy Qur‘an, Madinah Munawrah, Saudi Arabia. Pp: 525.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.