Active Electrode Poles (AEP): Do they Influence Outcomes of Sacral Nerve Modulation (SNM) in Patients Treated for Faecal Incontinence
by M Morales-Cruz, Y Persto, J Hayes, A Bagul*
Department of Surgery, Pelvic Floor, Queen Elizabeth Hospital, Birmingham UK
*Corresponding Author: Anil Bagul, Department of Surgery, Pelvic Floor, Queen Elizabeth Hospital, Birmingham UK
Received Date: 10 April 2026
Accepted Date: 17 April 2026
Published Date: 20 April 2026
Citation: Morales-Cruz M, Persto Y, Hayes J, Bagul A (2026) Active Electrode Poles (AEP): Do they Influence Outcomes of Sacral Nerve Modulation (SNM) in Patients Treated for Faecal Incontinence. J Surg 11: 11612DOI: https://doi.org/10.29011/2575-9760.011612
Abstract
Background: SNM is effective for patients with Faecal Incontinence (FI) failing conservative management. Currently a standardised method is followed at insertion. A decrease in the total motor threshold can be attained with 4 Active Electrode Poles (AEP), however this does not influence the therapeutic function. There is limited information on whether the final outcome of SNM is influenced by the total number of AEP at lead placement.
Aim: The primary aim was to analyse if the outcome was related to number of AEP achieved at lead insertion. Secondary points were to assess correlation between number of AEP, patient incontinence scores, health scores and follow up outcome.
Methods: Fifty one patients who underwent permanent implantation were included. All patients underwent a tined lead insertion (curved stylet 3889 Medtronic) using the standardised technique of lead placement. All patients had number of AEP along with baseline and follow up motor threshold documented.
Results: 37(76%) had 4 working AEP, the median threshold was 0.8 (0.3-2.8) mv. Our analysis showed no significant association between the number of working electrodes (AEP 0, 1, 2, 3), decreased stimulation amplitude on the Health (HS) and St. Marks score (SMIS), nor did they significantly alter follow up clinic visits.
Conclusions: A good functional outcome was achieved with optimised placement of lead but this was not influenced by the number of AEP, there was no significant decrease in follow up clinic visits for reprogramming. However 4 AEP suggest optimal lead placement, improved programming possibilities in turn leading to decreased stimulation amplitude and increase the battery longevity; long term follow up is required.
Introduction
Sacral Neuromodulation (SNM) was developed in the early 1980s by Tanagho and Schmidt [1], it was accepted by the FDA in 1997 [2] and the implantation technique commonly used today was described in 2003 by Spinelli et al.[3]. Sacral neuromodulation is considered the last available resource after the failure of conservative measures for bladder dysfunction and as first-line treatment for faecal incontinence. The review done by Janssen et al showed that 79% (69%- 83%) of patients experience an improvement of 50% or more in the number of weekly episodes of faecal incontinence at 12 months, and the percentage increases to 84% of patients after more than 36 months of follow-up [4]. The original device was modified in 2006, when its size was reduced to a half and leads were changed to decrease its chance of migration [5]. Three tined lead electrodes of different lengths (28, 33, and 41 cm) are available (Medtronic 3889-28, 3889-33, 3889- 41). These have four contact points (numbered 0, 1, 2, and 3 from distal to proximal) and a curved tip [6]. Proper patient selection and optimal electrode lead placement are the key determinants of success. The electrode configuration with the best sensory response at the lowest amplitude is chosen for therapeutic stimulation [7].
Methods
This study consists of a retrospective analysis of a prospectively collected database of patients undergoing sacral neuromodulation for treatment of faecal incontinence carreid out at a University teaching hospital by a single implanter. All pateints were demeed suitable for SNM having been discussed at the regional pelvic floor MDT. A total of 51 patients underwent tined lead implantation (curved stylet 3889 Medtronic); six patients were excluded from the analysis because of incomplete data. All the patients enrolled were assessed before and after the procedure according to the St. Mark’s incontinence score and the Health Score. This is an observational practice review, which reports the single consultant outcome data following SNS implantation within the context of their routine clinical practice. The project was conducted as part of internal practice review and registered as an audit study at the Queen Elizabeth Hospital Birmingham, United Kingdom (CARMS: 16232). Two non-parametric tests were employed to assess the differences between groups according to the number of active poles, Wilcoxon Signed Rank Test and Kruskal-Wallis Test. Statistical significance was considered with p-values of less than 0.05. Analysis was made IBM Statistical Package for the Social Sciences version 21.0 (IBM SPSS Inc., Chicago, IL, USA)
Results
Forty-three of patients included were female (95.5%). The mean age of population was 57.86 ± 14.24 years. Twenty six of the patients (57.7%) correlated their faecal incontinence with obstetric injuries. The median of St. Mark´s score before implantation was 18 (14-24) before the implantation and 13 postimplant. The mean for the Health Score (HS) was 54.42 (30-89) and 62.11 (20-80) respectively. There was a generalized improvement with only statistical significance reflected on health state (p= 0.001). The highest rank in HS was found in the group with 3 AEP’s with a mean of 36.85 (Figure 1). No statistical relevance was found in continence (p=0.77, Figures 2 and 3) Three devices were removed, one required a battery revision twice, one a lead revision and one reported problems with Impulse generator (IPG). Thirty-two (71.1%) patients had 4 AEP, ten patients (22.2%) had 3 and three (6.6%) had only 2 electrodes working. Currently the patients are being monitered for the longevity of the Implant Pulse Generator (IPG), currently none from the above cohort have been replaced over the last 6.5 years.
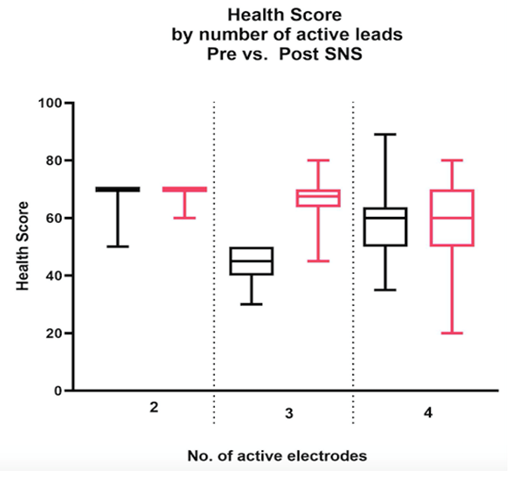
Table 1: Comparison of Health Scores before and after SNS implant with 2,3 and 4 AEPs.
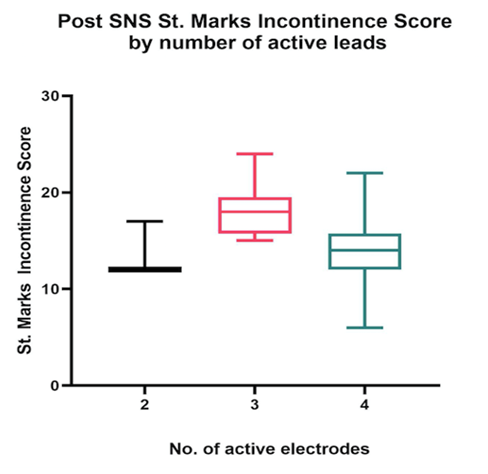
Table 2: Comparisons between St. Marks Incontinence Score depending on the number of AEPs.
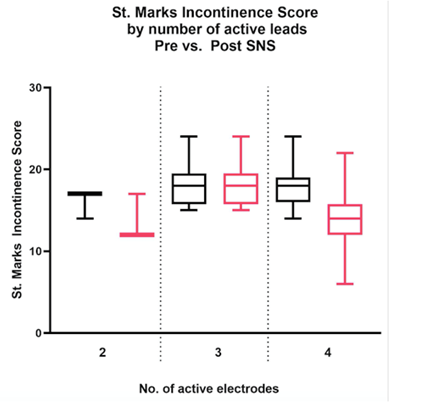
Table 3: Comparison of Pre and post St. Marks Scores corresponding to leads.
Discussion
Since the beginning of the use of SNM in the 1990s, four main programming parameters are considered essential to obtain a good therapy effect: the electrode configuration (selection of the anode and cathode), the amplitude of the electrical pulses (mA or V), the pulse frequency (Hz), and the pulse width (μs) which is the duration of each electrical pulse [7] Medtronic Inc. has developed two lead models, 3093 and 3889. Model 3093 has four equally 3 mm spaced 3 mm long electrodes at the distal end, numbered 0, 1, 2, and 3 starting at the tip. Model 3889 differs with electrode 2 being 10.2 mm long but continues with three 3 mm electrodes all spaced at 1.5 mm from the tip, all patients included in this study had the Model 3889 placed. Both models have a region with four tines spanning 15.5 mm. The start of the tined region is denoted by Marker Band A (spaced by 31mm from electrode 0) and the end of the tined region denoted by Marker Band B. Medtronic designed these markers to be an indication of lead depth during the percutaneous implantation process [6] The optimal placement aims to position the electrode with its four equally spaced contact points close to the target nerve (S3 or S4). A successful placement offers more programming options and reduces the intensity of stimulation, thus prolonging the battery life and lessening the risk of side effects [8]. The amplitude of stimulation determines the energy delivered to the sacral spinal nerve [9]. Precise lead placement allows for lower amplitude stimulation and low energy consumption to obtain the desired effect [10] The bellows response (an inward movement of the perineum) and ipsilateral toe/foot response (plantar flexion of the greater toe) confirm correct positioning. Stimulation intensities below 2 mA are the main goal [8]. Loss of efficacy refers to the reduction or loss of therapeutic effect of the SNM. Conservative options should be first attempted, but the electrodes and IPG should be checked for technical failure, which happens more commonly between the first 3 to 12 months after placement [11]. If no technical failure is found, the stimulation settings can be reprogrammed according to the algorithm of Dudding et al. [12]. Some have suggested changing the stimulation parameters whilst others have increased the number of Active Electrode Poles (AEPs) during tined lead placement [13] In the work published by Duelund-Jakobsen et al [14] in 2016 the functional results did not correlate to the number of active electrodes stimulated (p>0.05). The patients having an intraoperative motor response on stimulation of one, two, three and four poles were 18(9.7%), 75(40.3%), 61(32.8%) and 32(17.2%), respectively. All of them showed a satisfactory reduction of their Wexner Incontinence Score after a median follow up of 878 ±561 days. Assmann et al [15] performed a retrospective analysis in 2020 with the aim of correlating the number of AEPs during lead placement and the long-term efficacy of neuromodulation. The number of AEPs during lead placement was two (n = 42, 14.5%), three (n = 82, 28.5%) and four (n = 164, 57%) for a total population of 288 patients. The conclusion was a lack of association between the number of AEPs and the long-term efficacy of neuromodulation. Neither the success rate of the trial phase nor the battery life after first placed IPG was influenced by the number of AEPs.
Conclusions
Although the sample size of the study is small, it is shown that all groups achieved a good functional outcome despite the number of active electrode poles, and even when no statistical significance was found, the biggest variation on the St. Mark’s incontinence score was seen in the group of 4 AEPs. Four active electrodes also reflect a proper placement technique and offer a wider range of programming leading to decrease stimulation amplitude and increase the battery longevity. A larger study sample and follow up is needed to confirm any postive relation of number of AEP and outcome.
References
- Tanagho EA, Schmidt RA (1982) Bladder pacemaker: scientific basis and clinical future. Urology 20: 614 -619.
- https://www.meddeviceonline.com/doc/medtronic-announces-fda-approval-0001
- Spinelli M, Giardiello G, Gerber M, Arduini A, van den Hombergh U (2003) New sacral neuromodulation lead for percutaneous implantation using local anesthesia: description and first experience. J.Urol 170: 1905-1907.
- Janssen PTJ, Kuiper SZ, Stassen LPS, Bouvy ND, Breukink SO, et al. (2017) Fecal incontinence treated by sacral neuromodulation: long-term follow-up of 325 patients. Surgery 161: 1040-1048.
- Chughtai Bilal Thomas, Dominique; Sun, Tianyi; Sedrakyan, Art (2018) Failures of Sacral Neuromodulation for Incontinence JAMA Surgery.
- Medtronic Inc. Interstim Therapy 3093 3889 Implant Manual.2014:36. Medtronic, Inc.: Minneapolis, MN.
- Van Kerrebroeck PE, Marcelissen TA (2012) Sacral neuromodulation for lower urinary tract dysfunction. World J Urol 30: 445-450.
- Jacobs SA, Lane FL, Osann KE, Noblett KL (2014) Randomized prospective crossover study of interstim lead wire placement with curved versus straight stylet. Neurourol Urodyn 33: 488-492.
- Devane LA, Evers J, Jones JF, Ronan O’Connell P (2015) A review of sacral nerve stimulation parameters used in the treatment of faecal incontinence. Surgeon 13: 156-162.
- Rydningen MB, Dehli T, Wilsgaard T (2017) Sacral neuromodulation for faecal incontinence following obstetric sphincter injury—outcome of percutaneous nerve evaluation. Colorectal Dis 19: 274-282.
- Govaert B, Rietveld MP, van Gemert WG, Baeten CG (2011) The role of reprogramming in sacral nerve modulation for faecal incontinence. Colorectal Dis 13: 78-81.
- Dudding TC, Hollingshead JR, Nicholls RJ, Vaizey CJ (2011) Sacral nerve stimulation for faecal incontinence: optimizing outcomevand managing complications. Color Dis 13: e196-e202.
- Matzel KE, Chartier-Kastler E, Knowles CH (2017) Sacral neuromodulation: standardized electrode placement technique. Neuromodulation 20: 816-824.
- Duelund-Jakobsen J, Lundby L, Lehur PA, Wyart V, Laurberg S, et al. (2016) Is the efficacy of sacral nerve stimulation for faecal incontinence dependent on the number of active electrode poles achieved during permanent lead insertion? Colorectal Dis 18: O414-O419.
- Assmann R, Breukink SO, Caubergh SAP, Stassen LPS, van Kuijk SMJ et al. (2020) The effect of the number of active electro de poles during tined lead placement on longâterm efficacy of sacral neuromodulation in patients with faecal incontinence. Colorectal Disease, codi 15223.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.