Accuracy of The Twist Test for The Diagnosis of Unstable Triangular Fibrocartilage Complex Injury in The Wrist
by Maciej Piotrowski*, Filip Dąbrowski
Department of Orthopaedics and Kinetic Organ Traumatology, Medical University of Gdansk, Poland
*Corresponding author: Maciej Piotrowski, Medical University of Gdansk, Department of Orthopaedics and Kinetic Organ Traumatology Szpital Copernicus ul. Nowe Ogrody 1/6, 80-803 Gdansk, Poland.
Received Date: 09 April, 2026 Accepted Date: 21 April 2026 Published Date: 25 April 2026
Accepted Date: 21 April 2026 Published Date: 25 April 2026
Published Date: 25 April 2026
Citation: Piotrowski M, Dąbrowski F (2026) Accuracy of The Twist Test for The Diagnosis of Unstable Triangular Fibrocartilage Complex Injury in The Wrist. J Orthop Res Ther 11: 1421. DOI: https://doi.org/10.29011/2575-8241.001421
Abstract
Currently, there are no highly effective clinical tests for a TFCC injuries. Patients in whom existing tests do not indicate damage often report that wrist pain or symptoms occur only during complex wrist movements involving muscular tension or load. Therefore, we propose a new physical examination test, that replicates such complex movement. This research is intended to demonstrate the sensitivity and specificity of the new test in detecting of the unstable TFCC injury. Methods: The study utilised a clinical dataset comprising 109, patients aged 13-67 years old. Patients sample consisted of 75 TFCC-positive and 34 TFCC-negative outcomes. The test was classified as positive if the patient was unable to do it due to wrist’s pain or the test was painful, indicating a potential unstable TFCC injury. Arthroscopy was used to confirm TFCC injury, providing a definitive diagnosis through direct visualization of the intra-articular structures of the wrist. The sample size was deemed sufficient to estimate sensitivity and specificity with reasonable precision, based on guidelines for diagnostic test studies. Results: For unstable injuries, sensitivity was 72.9% with a specificity of 67.2%, PPV of 63.6%, and NPV of 75.9%. Among patients in the 25-35 years group within unstable injury strata, sensitivity peaked at 79.0% with specificity at 61,9%, for those above 35 years, sensitivity approximated 77.8% with specificity at 62,5%. Conclusion: The advantages of the Twist Test are high specificity and strong sensitivity for unstable injuries ensure accurate confirmation of TFCC injuries, particularly in patients above 25 years, making it effective for detecting severe TFCC pathology. It is very helpful in making decision whether arthroscopic treatment is necessary.
Keywords: Clinical Examination; TFCC; Wrist Injury; Wrist Pathology
Introduction
The triangular fibrocartilage complex (TFCC) is a structure located between the distal radius, ulna, and the carpus. It consists of the articular disc, the meniscus homologue, the dorsal and palmar radioulnar ligaments, the ulnolunate and ulnotriquetral ligaments, and the extensor carpi ulnaris tendon sheath [1,2]. TFCC functions as the primary stabilizer of the distal radioulnar joint (DRUJ) during forearm rotation and plays a crucial role in absorbing axial load at the wrist [2-4]. For these reasons, TFCC injuries can lead to DRUJ instability and ulnar-sided wrist pain [5]. Diagnosing the cause of ulnar-sided wrist pain or determining the specific type of TFCC injury is challenging. The ethology may be acute or chronic, and may involve damage to various ligaments or bones in the wrist. Missed diagnoses can result in persistent pain, instability, reduced grip strength, and decreased range of motion. Currently, there are no highly effective clinical tests for TFCC injuries. Physical examinations such as the ulnar fovea sign, the ulnocarpal stress test, and the ballottement test may aid in diagnosing TFCC injuries, but the limited by low specificity and sensitivity [6-11]. MRI is currently of limited value in evaluating the quality, mobility, and dynamic stability of the TFCC disc. Its accuracy in localizing TFCC injuries is very low. Negative MRI results or clinical provocative tests cannot reliably rule out the presence of clinically relevant TFCC tears [12,13]. At present, wrist arthroscopy is the only diagnostic tool capable of dynamically assessing the grade of instability and the healing potential of the injury [14-16]. Arthroscopy allows both diagnosis and treatment of TFCC injuries. However, it is an invasive procedure that disrupts tissue continuity, requires anaesthesia, and carries the risk of complications. Ideally, we would have more effective clinical tests that could safely and accurately identify TFCC damage requiring surgical intervention, without unnecessary exposure to diagnostic arthroscopy. Damage that does not destabilise the DRUJ can often be treated non-surgically [17]. Patients in whom existing tests do not indicate damage often report that wrist pain or symptoms occur only during complex wrist movements involving muscular tension or load. Therefore, we propose a new, effective physical examination test, that replicates such complex movement. For this purpose, we drew inspiration from hand movements in a children’s game popular in Polish kindergartens. Due to difficulties in literal translation, we have named it in English: The Twist Test.
Materials and Methods
In this cross-sectional observational study, we aimed to evaluate the diagnostic efficacy of the Twist Test for detecting unstable TFCC injuries in patients presenting wrist complaints. The study utilised a clinical dataset comprising 109, patients aged 13 - 67 years old, collected between 2019 - 2025. Patients sample consisted of 75 TFCC-positive and 34 TFCC-negative outcomes. The sample size was deemed sufficient to estimate sensitivity and specificity with reasonable precision, based on guidelines for diagnostic test studies [18]. The primary focus of the Twist Test was a clinical manoeuvre designed to assess the integrity of TFCC by applying complex movement to the wrist. The test was classified as positive if the patient was unable to do it due to wrist’s pain or the test was painful, indicating a potential TFCC injury. The primary outcome of the study was the presence or absence of an unstable TFCC injury, recorded as either positive or negative. Arthroscopy serves for confirming TFCC injury, providing a definitive diagnosis through direct visualization of the intra-articular structures of the wrist. All arthroscopies were performed by two experienced hand surgeons. Data on clinical test results and TFCC injury status were sourced from the arthroscopy findings, ensuring that arthroscopy, where performed, served as the definitive diagnostic benchmark. To mitigate potential biases, we addressed selection bias by including only patients with complete datasets, thereby minimising concerns related to missing data. Confounding factors such as age and injury type were explored through stratified analyses to elucidate their impact on test performance.
Technique of the Twist Test
(Figure1-2) The patient extends their hands in front of them so that the dorsal sides of both hands touch. The forearms lie one above the other. The patient interlaces their fingers - fifth finger of the left hand with the fifth of the right, fourth with fourth, and so on up to the index fingers - leaving the thumbs free. The lower forearm is in pronation and the upper forearm in supination (Figure 3). When the right forearm is lower, it is referred to as the right test; when the left is lower, it is the left test. The upper forearm is then rotated in the direction of pronation with simultaneous palmar flexion of both wrists (Figure 4). After bending the elbows, the forearms are rotated downwards and towards the chest. The final movement involves pulling the interlaced hands toward the chin, so that the forearms make contact with the chest. In this final position, the forearm that was initially on top now lies against the chest, and the lower forearm is positioned on top of it (Figure 5).
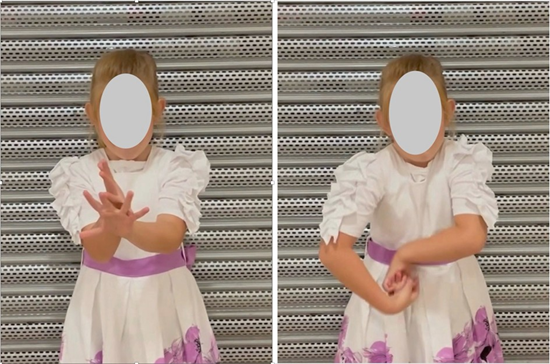
Figure 1: The child shows the Twist Test (left). The left photo: the child extends her hands in front of her so that the dorsal sides of both hands touch. The right photo: the upper forearm is then rotated in the direction of pronation with simultaneous volar flexion of both wrists.

Figure 2: The child shows the Twist Test (left). After bending the elbows, the forearms are rotated downwards and towards the chest. The final movement involves pulling the interlaced hands toward the chin, so that the forearms make contact with her chest.

Figure 3: A view from the perspective of the Twist Test (left) performer. The person extends her left hand. Next the dorsal sides of both hands touch. The forearms lie one above the other. She interlaces their fingers - fifth finger of the left hand with the fifth of the right, fourth with fourth, and so on up to the index fingers. The lower forearm is in pronation and the upper forearm is in supination. Later on, the upper forearm is then rotated in the direction of pronation.

Figure 4: A view from the perspective of the Twist Test (left) performer. After the upper forearm is rotated, both forearms are in the pronation position. Then she makes volar flexion of both wrists.
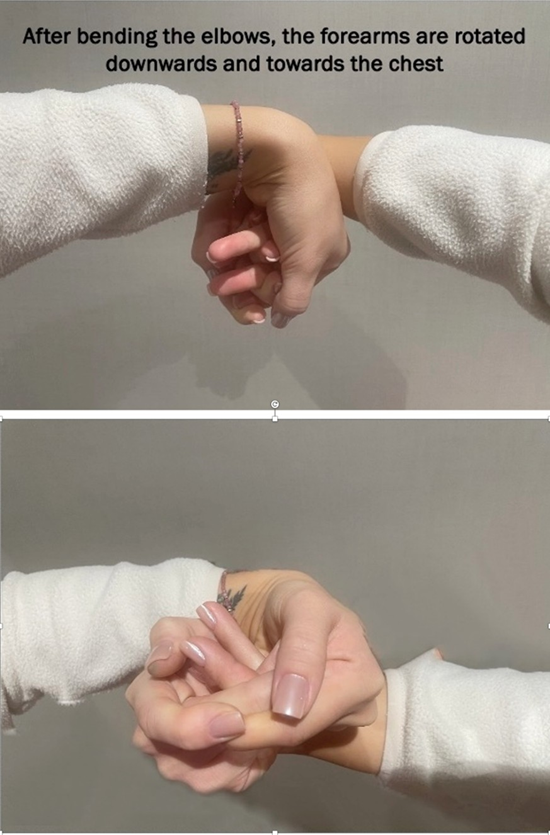
Figure 5: A view from the perspective of the Twist Test (left) performer. After bending the elbows, the forearms are rotated downwards and towards the performer’s chest. The final movement involves pulling the interlaced hands toward the chin, so that the forearms make contact with the chest.
Statistical analysis
The primary objective of this study was to evaluate the diagnostic performance of the Twist Test as a predictor of TFCC injury in patients with wrist pathology, including assessments of sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and contingency table metrics (true positives, false positives, true negatives, false negatives). Secondary objectives included:
- Stratifying the diagnostic performance by TFCC injury stability status (stable, unstable, and overall).
- Examining variations in diagnostic metrics across age groups (below 25 years, 25 - 35 years, and above 35 years) within each stability status.
- Assessing the association between the Twist Test results on a specific hand side and the ipsilateral or contralateral affected side to determine its predictive value for laterality.
A significance level of α = 0.05 was adopted, with p-values < 0.05 considered statistically significant, maintaining a 5% threshold for type I error in hypothesis testing. Analyses were conducted using the R Statistical language (version 4.3.3; R Core Team, 2024) on Windows 11 x64 (build 26100). The results were presented in tables and interpreted in accordance with the STROBE guidelines [19].
Results
Table 1 presents the demographic characteristics, clinical test results, ligament status, and TFCC pathology findings for a cohort of 109 patients with suspected wrist pathology, both overall and across age-stratified subgroups (Table 1).
|
Characteristic |
Overall (N=109) |
Below 25 Years (N=35) |
25-35 Years (N=40) |
Above 35 Years (N=34) |
p-value |
|
Demographics |
|||||
|
Dominant Hand |
1 |
||||
|
- Left |
3 (2.8%) |
1 (2.9%) |
1 (2.5%) |
1 (2.9%) |
|
|
- Right |
106 (97.2%) |
34 (97.1%) |
39 (97.5%) |
33 (97.1%) |
|
|
Affected Side |
0.32 |
||||
|
- Left |
37 (33.9%) |
14 (40.0%) |
10 (25.0%) |
13 (38.2%) |
|
|
- Right |
72 (66.1%) |
21 (60.0%) |
30 (75.0%) |
21 (61.8%) |
|
|
Clinical Tests |
|||||
|
The Twist Test (Right) |
0.051 |
||||
|
- Negative |
63 (57.8%) |
26 (74.3%) |
19 (47.5%) |
18 (52.9%) |
|
|
- Positive |
46 (42.2%) |
9 (25.7%) |
21 (52.5%) |
16 (47.1%) |
|
|
The Twist Test (Left) |
0.039 |
||||
|
- Negative |
72 (66.1%) |
29 (82.9%) |
23 (57.5%) |
20 (58.8%) |
|
|
- Positive |
37 (33.9%) |
6 (17.1%) |
17 (42.5%) |
14 (41.2%) |
|
|
TFCC pathology |
|||||
|
TFCC Injury |
0.215 |
||||
|
- Negative |
34 (31.2%) |
14 (40.0%) |
13 (32.5%) |
7 (20.6%) |
|
|
- Positive |
75 (68.8%) |
21 (60.0%) |
27 (67.5%) |
27 (79.4%) |
|
|
TFCC DRUJ Instability |
0.17 |
||||
|
- Stable |
61 (56.0%) |
24 (68.6%) |
21 (52.5%) |
16 (47.1%) |
|
|
- Unstable |
48 (44.0%) |
11 (31.4%) |
19 (47.5%) |
18 (52.9%) |
|
|
TFCC Injury (Palmer Classification) |
|||||
|
- IA: Central Perforation (Stable) |
27 (24.8%) |
9 (25.7%) |
9 (22.5%) |
9 (26.5%) |
0.914 |
|
- IB: Ulnar Avulsion (Unstable) |
20 (18.3%) |
2 (5.7%) |
8 (20.0%) |
10 (29.4%) |
0.037 |
|
- IC: Distal Avulsion (Unstable) |
21 (19.3%) |
5 (14.3%) |
10 (25.0%) |
6 (17.6%) |
0.482 |
|
- ID: Radial Avulsion (Unstable) |
16 (14.7%) |
6 (17.1%) |
2 (5.0%) |
8 (23.5%) |
0.055 |
|
- II: Degenerative (Subtypes IIA-IID, Variable stability) |
10 (9.2%) |
2 (5.7%) |
2 (5.0%) |
6 (17.6%) |
0.163 |
|
Notes: Footnotes p-values were calculated using Fisher’s exact test or Pearson’s Chi-squared test to assess differences across age categories. A p-value < 0.05 indicates statistical significance. TFCC Injury (Palmer Classification) percentages reflect patients with specific injury types; some patients may have multiple Palmer types, but totals are reported per category. |
|||||
Table 1: Characteristics of wrist pathology in patients with suspected TFCC injury: overall and age-stratified analysis
Overall sensitivity was 65.3%, reflecting a reasonable capacity to detect true positives, whereas specificity reached 82.4%, indicating robust performance in ruling out non-injured cases. Stratification by TFCC injury stability status, as per the first secondary objective, unveiled nuanced variations in test performance. For unstable injuries, sensitivity increased to 72.9%, coupled with a specificity of 67.2%, PPV of 63.6%, and NPV of 75.9%, with contingency counts showing 35 true positives and 13 false negatives. In contrast, stable injuries exhibited reduced sensitivity at 51.9% and specificity at 50.0%. This pattern demonstrates that the Twist Test may be more attuned to detecting unstable TFCC lesions (Table 2).
|
TFCC stability statusd |
Sensitivity, % (95% CI)e |
Specificity, % (95% CI)e |
PPV, % (95% CI)e |
NPV, % (95% CI)e |
TP |
FP |
TN |
FN |
|
Both stable and unstable |
49/75 (65.3) (54.1 - 75.1) |
28/34 (82.4) (66.5 - 91.7) |
49/55 (89.1) (78.2 - 94.9) |
28/54 (51.9) (38.9 - 64.6) |
49 |
6 |
28 |
26 |
|
Unstable |
35/48 (72.9) (59.0 - 83.4) |
41/61 (67.2) (54.7 - 77.7) |
35/55 (63.6) (50.4 - 75.1) |
41/54 (75.9) (63.1 - 85.4) |
35 |
20 |
41 |
13 |
|
Stable |
14/27 (51.9) (34.0 - 69.3) |
41/82 (50.0) (39.4 - 60.6) |
14/55 (25.5) (15.8 - 38.3) |
41/54 (75.9) (63.1 - 85.4) |
14 |
41 |
41 |
13 |
|
Notes: a The twist test refers to the clinical maneuver involving forearm rotation to assess for pain or instability indicative of TFCC injury. b TFCC, triangular fibrocartilage complex. c Data derived from 109 patients evaluated for wrist pathology, with TFCC injury confirmed via reference standard (e.g., arthroscopy). d the positive class for each category is the presence of the specified TFCC injury type versus all others (e.g., for “unstable,” positive = unstable injury, negative = stable injury or no injury). A positive twist test result is considered the predictor for the positive class of TFCC injury. e Percentages are calculated from raw counts, with 95% confidence intervals (CIs) computed using the Wilson score method. Abbreviations: PPV, positive predictive value; NPV, negative predictive value; TP, true positive; FP, false positive; TN, true negative; FN, false negative. |
||||||||
Table 2: Diagnostic performance metrics of the Twist Test for predicting TFCCb injury stratified by stability status (N = 109)c
Further exploration of age-related differences, addressing the second secondary objective, highlighted heterogeneous diagnostic accuracy across subgroups. Within unstable injury strata, sensitivity peaked at 79.0% with specificity 61,9% in the 25 - 35 years group. Slightly worse results were achieved in the group above 35 years with sensitivity 77.8% and specificity 62,5% (Table 3).
|
TFCC stability statusd |
Age group |
N |
Sensitivity, %(95% CI)e |
Specificity, %(95% CI)e |
PPV, %(95% CI)e |
NPV, %(95% CI)e |
TP |
FP |
TN |
FN |
|
Both stable and unstable |
Below 25 yrs. |
35 |
10/21 (47.6) (28.3 - 67.6) |
12/14 (85.7) (60.1 - 96.0) |
10/12 (83.3) (55.2 - 95.3) |
12/23 (52.2) (33.0 - 70.8) |
10 |
2 |
12 |
1 |
|
25–35 yrs. |
40 |
20/27 (74.1) (55.3 - 86.8) |
10/13 (76.9) (49.7 - 91.8) |
20/23 (87.0) (67.9 - 95.5) |
10/17 (58.8) (36.0 - 78.4) |
20 |
3 |
10 |
7 |
|
|
Above 35 yrs. |
34 |
19/27 (70.4) (51.5 - 84.1) |
6/7 (85.7) (48.7 - 97.4) |
19/20 (95.0) (76.4 - 99.1) |
6/14 (42.9) (21.4 - 67.4) |
19 |
1 |
6 |
8 |
|
|
Unstable |
Below 25 yrs. |
35 |
6/11 (54.5) (28.0 - 78.7) |
18/24 (75.0) (55.1 - 88.0) |
6/12 (50.0) (25.4 - 74.6) |
18/23 (78.3) (58.1 - 90.3) |
6 |
6 |
18 |
5 |
|
25–35 yrs. |
40 |
15/19 (79.0) (56.7 - 91.5) |
13/21 (61.9) (40.9 - 79.2) |
15/23 (65.2) (44.9 - 81.2) |
13/17 (76.5) (52.7 - 90.4) |
15 |
8 |
13 |
4 |
|
|
Above 35 yrs. |
34 |
14/18 (77.8) (54.8 - 91.0) |
10/16 (62.5) (38.6 - 81.5) |
14/20 (70.0) (48.1 - 85.5) |
10/14 (71.4) (45.4 - 88.3) |
14 |
6 |
10 |
4 |
|
|
Stable |
Below 25 yrs. |
35 |
4/10 (40.0) (16.8 - 68.7) |
17/25 (68.0) (48.4 - 82.8) |
4/12 (33.3) (13.8 - 60.9) |
17/23 (73.9) (53.5 - 87.5) |
4 |
8 |
17 |
6 |
|
25–35 yrs. |
40 |
5/8 (62.5) (30.6 - 86.3) |
14/32 (43.7) (28.2 - 60.7) |
5/23 (21.7) (9.7 - 41.9) |
14/17 (82.3) (59.0 - 93.8) |
5 |
18 |
14 |
3 |
|
|
Above 35 yrs. |
34 |
5/9 (55.6) (26.7 - 81.1) |
10/25 (40.0) (23.4 - 59.3) |
5/20 (25.0) (11.2 - 46.9) |
10/14 (71.4) (45.4 - 88.3) |
5 |
15 |
10 |
4 |
|
|
Notes: c Data derived from 109 patients evaluated for wrist pathology, with TFCC injury confirmed via reference standard (e.g., arthroscopy). Subgroup N values represent patients within each age category across the cohort. d the positive class for each category is the presence of the specified TFCC injury type versus all others (e.g., for “unstable,” positive = unstable injury, negative = stable injury or no injury). A positive twist test result is considered the predictor for the positive class. e Percentages are calculated from raw counts, with 95% confidence intervals (CIs) computed using the Wilson score method. Abbreviations: PPV, positive predictive value; NPV, negative predictive value; TP, true positive; FP, false positive; TN, true negative; FN, false negative |
||||||||||
Table 3: Diagnostic performance metrics of the Twist Test for predicting TFCC injury stratified by stability status and age groupc
The Twist Test (Right) demonstrates moderate sensitivity (56.0%) but high specificity (88.2%) and PPV (91.3%) in the overall sample. This suggests the test is effective in confirming TFCC injuries when positive, though it misses a substantial proportion of true cases (33 false negatives). The left-sided test has lower sensitivity (45.3%) but comparable specificity (91.2%) and PPV (91.9%). Evaluation of the Twist Test’s ability to predict laterality, fulfilling the third secondary objective, revealed modest concordance between test positivity on a specific hand side and the ipsilateral or contralateral affected side. In predicting the ipsilateral affected side - for the right hand, sensitivity was 45.8% and specificity 64.9%. Comparable metrics emerged for the left hand, including sensitivity of 45.9% and specificity of 72.2%. In predicting the contralateral affected side - for the right hand, sensitivity was 35.1% and specificity 54.2%. Comparable metrics emerged for the left hand, including sensitivity of 27.8% and specificity of 54.1%. Overall, these results imply limited lateralizing precision, advising integration with additional clinical assessments for accurate side localization (Table 4).
|
Tested hand sided |
Sensitivity, % (95% CI)e |
Specificity, % (95% CI)e |
PPV, % (95% CI)e |
NPV, % (95% CI)e |
TP |
FP |
TN |
FN |
|
Right ipsilateral |
33/72 (45.8) (34.8 - 57.3) |
24/37 (64.9) (48.8 - 78.2) |
33/46 (71.7) (57.5 - 82.7) |
24/63 (38.1) (27.1 - 50.4) |
33 |
13 |
24 |
39 |
|
Left ipsilateral |
17/37 (45.9) (31.0 - 61.6) |
52/72 (72.2) (61.0 - 81.2) |
17/37 (45.9) (31.0 - 61.6) |
52/72 (72.2) (61.0 - 81.2) |
17 |
20 |
52 |
20 |
|
Left contralat. |
20/72 (27.8) (18.8 - 39.0) |
20/37 (54.1) (38.4 - 69.0) |
20/37 (54.1) (38.4 - 69.0) |
20/72 (27.8) (18.8 - 39.0) |
20 |
17 |
20 |
52 |
|
Right contralat. |
13/37 (35.1) (21.8 - 51.2) |
39/72 (54.2) (42.7 - 65.2) |
13/46 (28.3) (17.3 - 42.5) |
39/63 (61.9) (49.6 - 72.9) |
13 |
33 |
39 |
24 |
|
Notes: c Data derived from 109 patients evaluated for wrist pathology. Metrics evaluate the association between a positive twist test result on the specified hand side and the affected side being the same (ipsilateral) or the affected side being the opposite (contralateral). d The positive class is the affected side matching the tested hand side. The positive class is the affected side being contralateral to the tested hand side. A positive twist test result on the tested side is considered the predictor for the positive class. e Percentages are calculated from raw counts, with 95% confidence intervals (CIs) computed using the Wilson score method. Abbreviations: PPV, positive predictive value; NPV, negative predictive value; TP, true positive; FP, false positive; TN, true negative; FN, false negative. |
||||||||
Table 4: Diagnostic performance metrics of the Twist Test performed on a specific hand side for predicting the ipsilateral and contralateral affected side (N = 109)c
Discussion
The triangular fibrocartilage complex (TFCC) is an anatomically complex structure spanning the radius, ulna, and carpus. Numerous biomechanical studies have demonstrated that it plays a vital role in absorbing axial load at the wrist and stabilising distal radioulnar joint (DRUJ) [2, 3]. Consequently, TFCC tears can result in DRUJ instability and ulnar-sided wrist pain. Several clinical examination techniques and special tests have been described in the literature to support the diagnosis of a suspected TFCC injury [20]. These tests can assist in identifying TFCC tear; however, their utility is limited by insufficient specificity and sensitivity [6-11,20]. Radiological investigations likewise have not demonstrated sufficient sensitivity and specificity to reliably detect TFCC injury [21]. Even MRI has limited value in assessing the structural integrity and dynamic stability of TFCC. This diagnostic uncertainty often necessitates further evaluation via wrist arthroscopy [22]. Wrist arthroscopy allows both diagnosis and treatment of TFCC injuries. It is the only diagnostic modality capable of evaluating injuries dynamically and assessing the extent of partial tears. However, it is an invasive procedure that requires anaesthesia and carries the risk of complications associated with surgical intervention and anaesthetic exposure. Additionally, the diagnostic accuracy of arthroscopy may be affected by variability in surgical experience [23]. Despite these limitations, wrist arthroscopy remains the gold standard for the identification of TFCC injuries [14-16]. It is well established that not all TFCC injury require surgical intervention. Damage that does not destabilise DRUJ can be effectively managed non-surgically [17]. Therefore, the aim of this study was to identify a clinical test involving complex wrist movement that could detect TFCC tears which destabilise DRUJ and thus require surgical treatment, including arthroscopy and TFCC repair. A reliable test of this kind would help reduce the number of unnecessary diagnostic arthroscopies and avoid exposing patients to the associated risk of surgical complications. With these objectives in mind, we began using the Twist Test in 2018.
Its promising effectiveness in recognising TFCC rupture that destabilise DRUJ prompted the initiation of this clinical study. The present analysis includes patients operated on in our department between 2019 and 2024. Patients qualified for wrist arthroscopy underwent both were right- and left-sided The Twist Test. Subsequently, wrist arthroscopy was performed to verify the accuracy of the test results.Overall sensitivity was 65.3%, reflecting a reasonable capacity to detect true positives, whereas specificity reached 82.4%, indicating robust performance in ruling out non-injured cases. PPV stood at 89.1%, underscoring high reliability when the test yielded a positive result, although NPV was lower at 51.9%, revealing limitations in excluding injury with a negative outcome. Whereas, taking into account the stability status of TFCC injury, unveiled variations in test performance. For stable IA injuries (central perforation), the Twist Test demonstrated limited diagnostic sensitivity across all assessments [3]. Overall sensitivity was 51.9%, with a specificity of 50%. These results suggest the Twist Test has limited utility in detecting stable IA injuries, with a tendency to miss many cases which reduces its diagnostic precision for this injury type. In contrast, the Twist Test performed notably better in identifying unstable TFCC injuries (IB - ID) [3]. Overall sensitivity was 72.9%, with a specificity of 67.2%. These metrics indicate that the Twist Test is more effective in detecting unstable TFCC injuries, potentially due to substantial biomechanical instability eliciting much clearer clinical signs during the maneuverer. It demonstrates improved sensitivity and specificity compared to its performance in stable injuries. Overall, these findings imply that the Twist Test is best suited for identifying unstable TFCC injuries, especially in clinical settings where significant pathology is suspected.
Taking into account the influence of patient age on diagnostic utility, the Twist Test was found to be most effective in identifying unstable TFCC injuries in individuals age 25-35 years, achieving a highest sensitivity of 79% and specificity of 61,9%. Slightly worse results were achieved in the group above 35 years demonstrating sensitivity 77.8%, high specificity 62,5% and strong PPV (70%). These metrics make it an initial clinical tool for detecting TFCC injuries in this demographic. Among patients below 25 years, sensitivity was 54,5% with specificity at 75%. These findings could suggest age-dependent influences, such as variations in tissue resilience, injury prevalence, or joint hypermobility more prevalent in patients below the age of 20 [24]. Cautious interpretation of the Twist Test in this group is advised, as reduced sensitivity compared to other age groups could result in an increased number of false negatives, meaning that the injury could be missed due to compensation from factors listed above. These findings suggest that TFCC injuries may be more detectable in patients aged above 25 years. The test was particularly effective at identifying unstable TFCC injuries, where it demonstrated a high capacity for detecting pathology that destabilises DRUJ but not helpful for distinguishing specific Palmer subtypes [3]. Clinically, the Twist Test should be prioritised in active patients aged above 25 years with a history of trauma or repetitive wrist stress, due to its hight sensitivity (79% and 77,8%). Evaluation of the Twist Test’s ability to predict laterality revealed modest concordance between test positivity on a specific hand side and the ipsilateral or contralateral affected side. Overall, results imply limited precision when only one test is used (the Twist Test right or left). Base on the statistical analysis, we recommend using both the Twist Test (right and left) when possible. This feature of the Twist Test could be an interesting topic for further studies. The limitations of the Twist Test include moderate sensitivity in certain age group (e.g., below 25), and for stable TFCC injuries. However, since stable injuries are typically less symptomatic and respond well to conservative treatment, failure to detect them may have minimal impact on clinical outcomes [3, 17]. Another limitation is the low specificity for distinguishing specific Palmer subtypes, reducing the test’s value for precise classification of TFCC injuries. It is important to remember that the Twist Test was developed specifically to detect unstable lesion that require arthroscopic treatment. Therefore, its utility lies in identifying clinically significant injuries, not necessarily all types of TFCC pathology. A minor drawback is that some patients may struggle to perform the test, but notably, the manoeuvre originates from a children’s game common in Polish kindergartens, and can usually be performed by children as young as 6. The advantages of the Twist Test are high specificity and strong sensitivity for unstable injuries ensure accurate confirmation of TFCC injuries, particularly in patients above 25 years, making it effective for detecting severe TFCC pathology. It is very helpful in making decision whether arthroscopic treatment is necessary. The other advantage of this test is the fact that this clinical examination is non-invasive and touch-free. The Twist Test can by performed remotely, enabling telemedicine applications, which are increasingly relevant in the context of pandemics, conflict zones, or limited access to hand surgery specialists.
Conclusion
The advantages of the Twist Test are high specificity and strong sensitivity for unstable injuries ensure accurate confirmation of TFCC injuries, particularly in patients above 25 years, making it effective for detecting severe TFCC pathology. It is very helpful in making decision whether arthroscopic treatment is necessary.
Conflict of Interest
No benefits in any form have been received or will be received related directly or indirectly to the subject of this article.
References
- Abe Y, Tominaga Y, Yoshida K (2012) Various patterns of traumatic triangular fibrocartilagecomplex tear. Hand Surg 17(2): 191-198.
- Nakamura T, Yabe Y, Horiuchi Y (1996) Functional anatomy of the triangular fibrocartilage complex. Journal of hand surgery 21(5): 581586.
- Palmer Ak (1989) Triangular fibrocartilagecomplex lesions: a classification. J Hand Surg Am 14(4): 594–606.
- Atzei A (2009) New trends in arthroscopic management of type 1-B TFCC injurieswith DRUJ instability. J Hand Surg Eur 34(5): 582-591.
- Palmer AK (1990) Triangular fibrocartilage disorders: injury patterns and treatment. Arthroscopy 6(2): 125-132.
- Ou Yang O, McCombe DB, Keating C, Maloney PP, Berger AC, et al. (2021) Ulnar-sided wrist pain: a prospective analysis of diagnostic clinical tests. ANZ J Surg (10): 2159-2162.
- Tay SC, Tomita K, Berger RA (2007) The “ulnar fovea sign” for defining ulnar wrist pain: an analysis of sensitivity and specificity. J Hand Surg Am 32(4): 438-444.
- Kirchberger MC, Unglaub F, Mühldorfer-Fodor M, Pillukat T, Hahn P, et al. (2015) Update TFCC:histology and pathology, classification, examination and diagnostics. ArchOrthop Trauma Surg 135(3): 427437.
- Jawed A, Ansari MT, Gupta V (2020) TFCC injuries: how we treat? J Clin Orthop Trauma 11(4): 570-579.
- Schmauss D, Pöhlmann S, Lohmeyer JA, Germann G, Bickert B, et al. (2016) linical tests and magnetic resonance imaging have limited diagnostic value for triangular fibrocartilaginous complex lesions. Arch Orthop Trauma Surg 136(6): 873-880.
- Moriya T, Aoki M, Iba K, Ozasa Y, Wada T, et al. (2009) Effect of triangular ligament tears on distal radioulnar joint instability and evaluation of three clinical tests: a biomechanical study. J Hand Surg Eur 34(2): 219-223.
- Andersson JK, Andernord D, Karlsson J, Fridén J (2014) Efficacy of Magnetic Resonance Imaging and Clinical Tests in Diagnostics of Wrist Ligament Injuries: A Systematic Review. Arthroscopy 31(10): 20.e2.
- Morley J, Bidwell J, Zachary M (2001) A comparison of the findings of wrist arthroscopy and magnetic resonance imaging in the investigation of wrist pain. J Hand Surg Br (6): 544-546.
- Mannil L, Martin W, Dahmen J, Witte T,Juten PG, et al. (2016) Arthroscopic treatment for ulnar-sided TFCC-tears. Eur J Trauma Emerg Surg 42(1): 29-35.
- Phillips R, Choo S, Fletcher B, Nuelle JAV (2023) Dry Wrist Arthroscopy: Technique and Rationale. Arthroscopy 39(8): 1779-1780.
- Petsatodis E, Pilavaki M, Kalogera A, Drevelegas A, Agathangelidis F, et al. (2019) Comparison between conventional MRI and MR arthrography in the diagnosis of triangular fibrocartilage tears and correlation with arthroscopic findings. Injury 50(8): 1464-1469.
- Choi SI, Malik S, MacLean S (2024) The Natural History of Nonoperatively Treated Traumatic Triangular Fibrocartilage Complex Tears: A Systematic Review. J Wrist Surg 13(6): 550-558.
- Bland JM (2015) An introduction to medical statistics (4th ed.). Oxford University Press.
- von Elm E, Altman D, Egger M, Pocock SJ, Gøtzsche PC, et al. (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). explanation and elaboration. Epidemiology 18(6): 805-835.
- Robb L, Rust P (2023) Accuracy of the Pisiform Boost Test for the Diagnosis of Triangular Fibrocartilage Complex Tears in the Wrist - Pisiform Boost Test. Arch Bone Jt Surg 11(2): 124-129.
- Hobby JL, Tom BD, Bearcroft PW, Dixon AK (2001) Magnetic resonance imaging of the wrist: diagnostic performance statistics. Clin Radiol Jan 56(1): 50-57.
- Andersson JK, Andernord D, Karlsson J, Fridén J (2014) Efficacy of Magnetic Resonance Imaging and Clinical Tests in Diagnostics of Wrist Ligament Injuries: A Systematic Review. Arthroscopy 31(10): 20.e2.
- Löw S, Prommersberger KJ, Pillukat T, van Schoonhoven J (2010) 10 Volume 11; Issue 02 J Orthop Ther, an open access journal ISSN: 2575-8241 Intra- und Interobserver-Reliabilität digital fotodokumentierter Befunde von Handgelenksspiegelungen [Intra- and interobserver reliability of digitally photodocumented findings in wrist arthroscopy]. Handchir Mikrochir Plast Chir 42(5): 287-292.
- Sobhani-Eraghi A, Motalebi M, Sarreshtehdari S, Molazem-Sanandaji von Handgelenksspiegelungen [Intra- and interobserver reliability of B, Hasanlu Z (2020) Prevalence of joint hypermobility in children and digitally photodocumented findings in wrist arthroscopy]. Handchir adolescents: A systematic review and meta-analysis. J Res Med Sci Mikrochir Plast Chir 42(5): 287-292. (25): 104.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.