A Silent Progression: A Case of Incidental Gallbladder Carcinoma in an 18-Year-Old Female
by Hadayat Ullah*
Senior House Officer Surgery, RCSI Hospitals, Cavan and Monaghan Hospital, Ireland
*Corresponding author: Hadayat Ullah, Senior House Officer Surgery, RCSI Hospitals, Cavan and Monaghan Hospital, Ireland
Received Date: 23 January 2025
Accepted Date: 28 January 2026
Published Date: 30 January 2026
Citation: Ullah H. (2026). A Silent Progression: A Case of Incidental Gallbladder Carcinoma in an 18-Year-Old Female. Ann Case Report. 11: 2515. https://doi.org/10.29011/2574-7754.102515
Abstract
Gallbladder cancer in children and adolescents is uncommon and remains undetected; until it becomes advanced, making it difficult to diagnose. We report the case of a female patient, aged18 years, who presented with features suggestive of gallstones. The patient underwent an uneventful laparoscopic cholecystectomy at a tertiary care. However, the pathology report was surprising and revealed moderately differentiated adenocarcinoma with substantial local invasion. This example is an obvious indicator that serious malignancy can occur even in young children with gallbladder disease that appears to be simple. This highlights the importance of Careful evaluation of gallbladder specimens and increases awareness that, despite being rare in young people, gallbladder cancer can strike suddenly.
Keywords: Gall Bladder; Rare Malignancy; Adenocarcinoma; Diagnostic Error; Cholecystectomy.
Introduction
The most prevalent cancer of biliary system is gallbladder carcinoma with adenocarcinoma being the predominant subtype which ranks fifth most common malignancy associated with the digestive track [1-3,21]. Although this cancer is relatively rare compared to other gastrointestinal malignancies, it carries a disproportionately poor prognosis due to its late presentation [2,18]. Among the established risk factors, gallstones are known to be the most significant. This increases in individuals with stones larger than 3 cm, long- standing cholelithiasis, and porcelain gall bladders. Other factors that contribute to increased susceptibility include a family history of gall bladder disease and female sex, likely due to hormonal influences and metabolic conditions such as cholesterol cycling [4-7,22-24] Chronic inflammations is another risk factor for carcinogenesis. Persistent mucosal irritation induces metaplasia, which progresses to dysplasia and eventually leads to malignant transformation [8].
Persistent infections with Helicobacter Pylori and Salmonella typhi, and some medications, such as contraceptive pills and isoniazid, raise the risk of GBC [8,14]. The overall prognosis is poor, and Patient with any stage of GBC have a reported 5-year survival of 12 %, which suggests silent progression and lack of screening strategies [9]. GBC can be clinically apparent and display signs of distant metastasis; however, in children, it may be accidentally found during a histological examination or laparotomy for other indications [10,19]. Epidemiological data also demonstrate marked variations in the incidence of GBC based on region and ethnicity. South Asian and Latin American populations, particularly women of South Asian and Hispanic origins, have shown higher incidence and mortality rates. Conversely, the prevalence in other parts of Asia and Europe is relatively low [11]. The subject of this case study was an 18-year-old female, who presented with features of gallstones, and a definitive diagnosis turned out to be gallbladder carcinoma.
Case Presentation
An 18 years old patient presented, complaining of abdominal discomfort of 1-month duration, particularly in the right upper quadrant. It was not associated with symptoms such as nausea, vomiting or anorexia. There were no constitutional signs such as fever, headache or weight loss. She had no prior medical history history including hemoglobinopathies. Clinical examination revealed mild tenderness in the right hypochondrium without any rigidity or guarding, and Murphy’s sign was negative. The pain was extensively investigated prior to admission. Ultrasound of abdomen and pelvis revealed a contracted, thick-walled gallbladder (6mm wall thickness) and a small 4 mm calculus in the right kidney’s inferior pole. The liver, pancreas, spleen, and other abdominopelvic structures were normal. Her blood investigations were unremarkable with Hemoglobin 10.2 g/dL, TLC 4,920/µL, Platelets 392,000/µL, Bilirubin 0.29 mg/dL, ALT 24 U/L, ALP 104 U/L. Her HBsAg, anti-HCV, and HIV were negative. Following the investigations, the patient underwent laparoscopic cholecystectomy for the diagnosis of symptomatic cholelithiasis. However, the operative findings were more complex than what was anticipated. The gallbladder contained stones and was fibrotic, puckered and densely adherent to the common bile duct (CBD). The pus became apparent in the cul-de-sac. The appendix was inflamed and contained a fecolith; therefore, an appendectomy was performed. The resected gallbladder and appendix specimens were subjected to histopathological analysis.
Analysis of the gallbladder specimen revealed moderately differentiated adenocarcinoma of grade 2, as shown in (Figure 1, 2). It was perforating the serosa along with extensive lymphatic, vascular and perineural invasion (pT3NxMx). Immunohistochemistry revealed positive results for CK7 and p53. Analysis of the appendix specimen revealed chronic granulomatous inflammation with fecoliths and no evidence of malignancy.
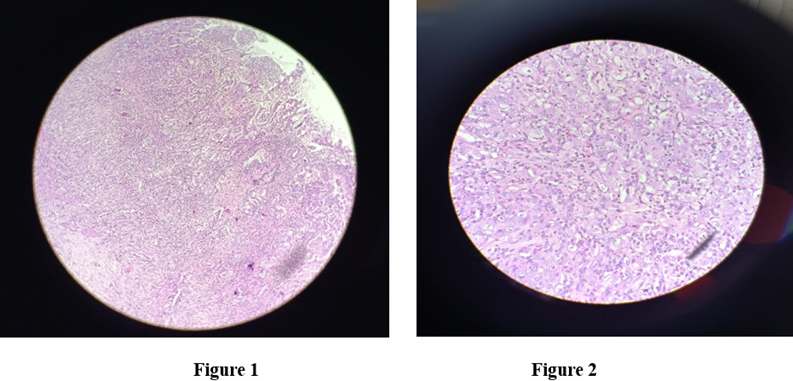
Figure 1 and Figure 2: Histopathology of the gallbladder showing moderately differentiated adenocarcinoma (H&E stain). High-power view showing malignant glandular structures with stromal invasion, consistent with adenocarcinoma (H&E stain).
On follow-up, the patient presented with features of obstructive jaundice; therefore, she was re-admitted and underwent MRCP followed by triphasic CT scan. As demonstrated by (Figure 3). The MRCP report revealed upper abdominal lymphadenopathy with a mass effect on the CBD, leading to cholestasis and altered signal intensity in segment IV of liver has left lobe.
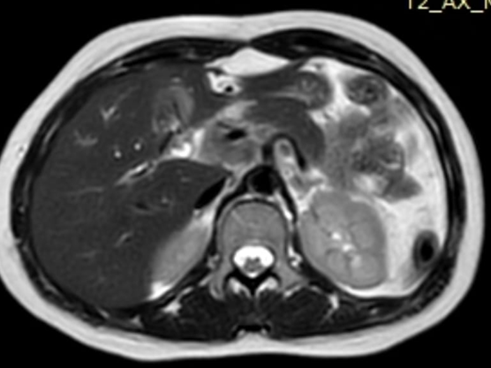
Figure 3: Bulky lymphadenopathy producing mass effect on the common bile duct, leading to obstructive cholestasis and secondary signal changes in segment IV of the left hepatic lobe.
The radiological findings of Triphasic CT scan were highly suggestive of metastatic lymphadenopathy from the primary gallbladder malignancy, causing obstructive cholestasis as shown in (Figure 4).
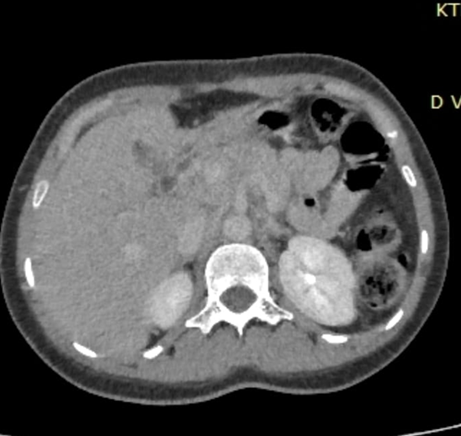
Figure 4: Suggestive of metastatic lymphadenopathy secondary to primary gallbladder carcinoma, causing obstructive cholestasis
Following up with the gastroenterology and cancer services was the patient’s discharge plan.
Discussion
Gallbladder cancer ranks fifth among digestive tract malignancies and is the most common biliary tract cancer. It primarily impacts elderly women and highest occurrence in the sixth and seventh decades [12]. Its occurrence in patients under 20 years as in our case, is extremely rare, which highlights the diagnostic challenge posed by this silent disease [8,13]. Gallstones, which are thought to be the most prevalent risk factors for GBC, were not linked to the reported cases of pediatric and adolescent GBC. Nevertheless, gallstones remain central to the pathogenesis of adult GBC, where chronic mechanical irritation of the mucosa caused by gallstones induces metaplasia, which progresses to dysplasia and ultimately to carcinoma. Other recognized factors contributing to GBC include obesity, Helicobacter pylori and Salmonella typhi infections, and drugs such as contraceptive pills [14,22]. Certain geographic and ethnic variations are also notable, suggesting the influence of environmental and genetic factors. It is strongly associated with female sex due to hormonal influences, particularly the role of high estrogen levels, and the higher incidence of gall stone formation [14,17,23-25].
Clinically, GBC is a silent masquerader for other disease. Vague presentations, such as right upper quadrant abdominal pain, abdominal discomfort, and dyspepsia, mimic benign diseases and delay suspicion of malignancy. Hence, more than two-thirds of patients are diagnosed late, after the condition has silently progressed to advanced stages where curative surgical options are limited [15,26]. In our patient, clinical and radiological findings were suggestive of simple cholelithiasis, but the true pathology emerged on histopathology. This underlines, the critical lesson of histopathological analysis of gall bladder specimens regardless of patient age, clinical suspicion, or intraoperative appearance [16,20].
Conclusion
Gallbladder carcinoma is rare but exceedingly aggressive malignancy that usually presents in elderly women, and is very uncommon in children and adolescents. This 18-year-old patient’s case demonstrated the silent progression of an unexpected malignancy that was initially mimicked by cholelithiasis. The incidental finding of moderately differentiated adenocarcinoma emphasizes the significance of histopathological analysis of the removed gallbladder specimens, irrespective of the patient’s age, clinical suspicion, and intraoperative findings.
Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following.
Funding: No financial support was received from any organization for the submitted work.
Contributions of authors: After reviewing final draft all authors agreed to take responsibility for publication.
Principal author; Hadayat Ullah; Concept and design: Hadayat Ullah; Drafting of the manuscript: Hadayat ullah; Critical review of the manuscript for important intellectual content: Hadayat Ullah
Disclosures Human subjects: Written informed Consent was taken
References
- Sahai P, Mall A, Yadav A, Yadav HP, Rastogi A, et al. (2025). Gallbladder cancer in a young male: An insight into an integrative approach for improving survival. Journal of Cancer Research and Therapeutics. 21: 720-724.
- Torre LA, Siegel RL, Islami F, Bray F, Jemal A. (2018). Worldwide burden of and trends in mortality from gallbladder and other biliary tract cancers. Clinical Gastroenterology and Hepatology. 16: 427-437.
- Goetze TO. (2015). Gallbladder carcinoma: Prognostic factors and therapeutic options. World Journal of Gastroenterology. 21: 12211-12217.
- Piehler JM, Crichlow RW. (1977). Primary carcinoma of the gallbladder. Archives of Surgery. 112: 26-30.
- Pilgrim CH, Groeschl RT, Christians KK, Gamblin TC. (2013). Modern perspectives on factors predisposing to the development of gallbladder cancer. HPB. 15: 839-844.
- Hsing AW, Bai Y, Andreotti G, Rashid A, Deng J, et al. (2007). Family history of gallstones and the risk of biliary tract cancer and gallstones: A population-based study in Shanghai, China. International Journal of Cancer. 121: 832-838.
- Miyazaki M, Takada T, Miyakawa S, Tsukada K, Nagino M, et al. (2008). Risk factors for biliary tract and ampullary carcinomas and prophylactic surgery for these factors. Journal of Hepato-Biliary-Pancreatic Surgery. 15: 15-24.
- Muduly DK, Satyanarayana Deo SV, Shukla NK, Kallianpur AA, Prakash R, et al. (2012). Gall bladder cancer in a child: A rare occurrence. Journal of Cancer Research and Therapeutics. 8: 653-654.
- Nishio H, Nagino M, Ebata T, Yokoyama Y, Igami T, et al. (2007). Aggressive surgery for stage IV gallbladder carcinoma: What are the contraindications? Journal of Hepato-Biliary-Pancreatic Surgery. 14: 351-357.
- Andrén-Sandberg A. (2012). Diagnosis and management of gallbladder cancer. North American Journal of Medical Sciences. 4: 293-299.
- Lazcano-Ponce EC, Miquel JF, Muñoz N, Herrero R, Ferrecio C, et al. (2001). Epidemiology and molecular pathology of gallbladder cancer. CA: A Cancer Journal for Clinicians. 51: 349-364.
- Rawla P, Sunkara T, Barsouk A. (2019). Epidemiology of colorectal cancer: Incidence, mortality, survival, and risk factors. Przeglad Gastroenterologiczny. 14: 89-103.
- Iwai N, Goto Y, Taniguchi H, Tokiwa K, Tsuto T, et al. (1985). Cancer of the gallbladder in a 9-year-old girl. Zeitschrift für Kinderchirurgie. 40: 106-107.
- Zatonski WA, Lowenfels AB, Boyle P, Maisonneuve P, Bueno de Mesquita HB, et al. (1997). Epidemiologic aspects of gallbladder cancer: A case-control study of the SEARCH Program of the International Agency for Research on Cancer. Journal of the National Cancer Institute. 89: 1132-1138.
- Andrén-Sandberg A. (2012). Diagnosis and management of gallbladder cancer. North American Journal of Medical Sciences. 4: 293-299.
- Singh A, Singh G, Kaur K, Goyal G, Saini G, et al. (2019). Histopathological changes in gallbladder mucosa associated with cholelithiasis: A prospective study. Nigerian Journal of Surgery. 25: 21-25.
- Kamisawa T, Ando H, Suyama M, Shimada M, Morine Y, et al. (2012). Japanese clinical practice guidelines for pancreaticobiliary maljunction. Journal of Gastroenterology. 47: 731-759.
- Ulanja MB, Moody AE, Beutler BD, Antwi-Amoabeng D, Rahman GA, et al. (2022). Early-onset pancreatic cancer: A review of molecular mechanisms, management, and survival. Oncotarget. 13: 828-841.
- Romano F, Franciosi C, Caprotti R, De Fina S, Porta G, et al. (2001). Laparoscopic cholecystectomy and unsuspected gallbladder cancer. European Journal of Surgical Oncology. 27: 225-228.
- Kumar S, Kumar S, Kumar S. (2006). Infection as a risk factor for gallbladder cancer. Journal of Surgical Oncology. 93: 633-639.
- Lazcano-Ponce EC, Miquel JF, Muñoz N, Herrero R, Ferrecio C, et al. (2001). Epidemiology and molecular pathology of gallbladder cancer. CA: A Cancer Journal for Clinicians. 51: 349-364.
- Diehl AK. (1983). Gallstone size and the risk of gallbladder cancer. JAMA. 250: 2323-2326.
- Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. (2003). Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. New England Journal of Medicine. 348: 1625-1638.
- Larsson SC, Wolk A. (2007). Obesity and the risk of gallbladder cancer: A meta-analysis. British Journal of Cancer. 96: 1457-1461.
- Toyonaga T, Chijiiwa K, Nakano K, Noshiro H, Yamaguchi K, et al. (2003). Completion radical surgery after cholecystectomy for accidentally undiagnosed gallbladder carcinoma. World Journal of Surgery. 27: 266-271.
- Braghetto I, Bastias J, Csendes A, Chiong H, Compan A, et al. (1999). Gallbladder carcinoma during laparoscopic cholecystectomy: Is it associated with bad prognosis? International Surgery. 84: 344-349.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.